Download
1 / 19
190 likes | 195 Vues
Caucasian Female With Dyslipidemia, Fatigue and Insulin Resistance. Primary Prevention

E N D
Caucasian Female With Dyslipidemia, Fatigue and Insulin Resistance Primary Prevention History of present illness: 58 year old female with history of high cholesterol on Simvastatin 20 mg without change for years. Also fatigued and having issues with ongoing weight gain despite a low calorie, low fat diet. Has been on diets for years and has struggled to lose weight. Has also had borderline glucose and pre-diabetes but no treatment in past. One doctor suggested bariatric surgery which is of no interest to her. She has high BP and not optimal control but taking medications listed. Cholesterol has been primarily high LDL.
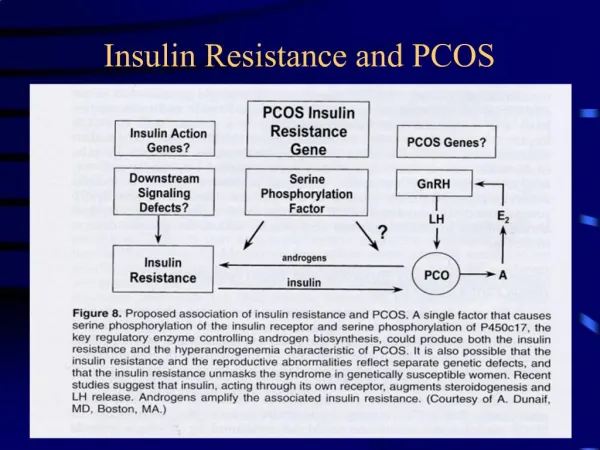
Questions to Consider • Question 1: Potential causes of fatigue? Severe Vitamin D deficiency, suboptimal thyroid treatment; Untreated insulin resistance? Sleep apnea? Depression? • Question 2: Currently on low calorie, low fat diet? Any previous trials of low carb diet and results? • Question 3: History of irregular menses? Hirsuitism? Infertility? Babies >9 pounds? Prior PCOS?
NMR LipoProfile • Insert NMR LipoProfile 02032011 KW52 Insert • Insert NMR LipoProfile 02032011 KW52 Page 2
Initial Treatment & Management • Advise home blood pressure meter • Start 50,000 IU vitamin D2/week and vitamin D3 5000 IU/day for severe vitamin D deficiency • Start metformin ER 500 mg 3-4 tablets daily with slow titration as tolerated over the next few weeks • Advised low carbohydrate diet and daily exercise • Consider work up for sleep apnea and depression
Follow Up • Vitamin D deficiency - improved with vitamin D supplementation and much less fatigue. • Impaired fasting glucose - improved with metformin 1000-1500 mg. HbA1c reduced. • Elevated lipoprotein(A) – no change • Essential hypertension – no change • Familial hypercholesterolemia - improved with insulin resistance treatment and diet change, continues simvastatin 20 mg.
NMR LipoProfile • Insert NMR LipoProfile 04192011 KW52 Insert • NMR LipoProfile 04192011 KW52 Page 2
Clinical Pearls It is important to always treat secondary causes of abnormal lipids. In this case LDL-P was elevated and no additional lipid medications were needed to completely normalize lipoproteins. Insulin resistance contributes to elevated small dense LDL and overall LDL-P and Apo B. Trial of low dose generic long acting metformin may be all that is needed. When prescribing Metformin use the generic long acting Metformin ER 500 mg is cheaper than 750 mg/day. I advise start with one for a few days to make sure no GI side effects. Then increase to 2 and eventually 3-4 for total dose of 2000 mg/day. We give script for Metformin ER 500 mg take 3-4 daily as tolerated. It will not produce hypoglycemia so safe to use in pre-diabetes. Lipoproteins shifts occur more on the higher dose of Metformin. In this patient she is taking only 1000 mg with intermittent 1500 mg and still had improvement.
References • Shimabukuro M, Higa M, Tanaka H, et al. Distinct effects of pitavastatin and atorvastatin on lipoprotein subclasses in patients with Type 2 diabetes mellitus. Diabet Med. Jul 2011;28(7):856-64. • Marcovina SM, Kennedy H, Bittolo Bon G, Cazzolato G, Galli C, Casiglia E, Puato M, Pauletto P (May 1999). "Fish intake, independent of apo(a) size, accounts for lower plasma lipoprotein(a) levels in Bantu fishermen of Tanzania: The Lugalawa Study". Arteriosclerosis, Thrombosis, and Vascular Biology 19 (5): 1250–6. doi:10.1161/01.ATV.19.5.1250. PMID 10323776. • Diagnosis and classification of diabetes mellitus. Diabetes Care. Jan 2010;33 Suppl 1:S62-9 • Standards of medical care in diabetes. Diabetes Care. Jan 2012;35 Suppl S20. • Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet. Sep 12 1998;352(9131):854-65. • KnowlerWC,Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM. Reduction in the incident of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393-403. • Gerstein HC, Yusuf S, Bosch J, Pogue J, Sheridan P, Dinccag N, Hanefeld M, Hoogwerf B, Laakso M, Mohan V, Shaw J, Zinman B, Holman RR. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomized controlled trial. Lancet 2006;368:1096-1105. • Orchard TJ, Temprosa M, Goldberg R, Haffner S, Ratner R, Marcovina S, Fowler S: The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: the Diabetes Prevention Program randomized trial. Ann Intern Med 2005; 142:611-619.