Download
1 / 70
780 likes | 1.49k Vues
Electrolyte Abnormalities in the Hospitalized Patient. Cynthia Seitz MD. Goals of the lecture. Discuss the electrolyte abnormalities in hospitalized child with respect to Sodium Potassium Phosphorus. Sodium Homeostasis. Sodium - dominant cation of extracellular fluid

E N D
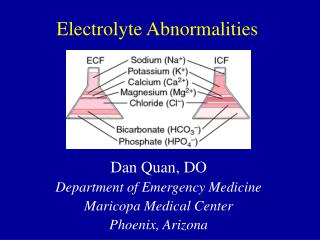
Electrolyte Abnormalities in the Hospitalized Patient Cynthia Seitz MD
Goals of the lecture • Discuss the electrolyte abnormalities in hospitalized child with respect to • Sodium • Potassium • Phosphorus
Sodium Homeostasis • Sodium - dominant cation of extracellular fluid • Principal determinant of extracellular osmolality. • The low intracellular sodium concentration, approximately 10 mEq/L, is maintained by Na+, K+-ATPase, which exchanges Na+ for K+ • Sodium is necessary for the maintenance of intravascular volume. • Sodium excretion occurs in stool and sweat, but the kidney regulates sodium balance and is the principal site of sodium excretion. • Plasma VOLUME- not osmolality determines the excretion of sodium by the kidney • renin-angiotensin-aldosterone system • In hyponatremia or hypernatremia, the underlying pathophysiology determines urinary Na+, not the serum sodium concentration • When extracellular sodium ↑’s→ plasma tonicity ↑→water efflux from cells →cellular dehydration (↓ cell volume) (to maintain equal osmolality inside and outside the cell) • Also ADH is released- renal conservation of water Sodium is unique among electrolytes… because water balance, not sodium balance, usually determines its concentration.
Hyponatremia The most common electrolyte abnormality in children: 1.5% of all pediatric hospitalizations Causes: • Increased Free water • Increased sodium loss • Decreased salt intake Most common cause in children is extra-renal GI losses like diarrhea.
Hyponatremia- types Hypovolemic Hyponatremia • Renal Loss: Urine Na > 20 mEq/L • Diuretic Use • Urinary tract obstruction and/or urinary tract infection • Autosomal recessive polycystic kidney disease • Tubulointerstitial nephritis • Cerebral salt wasting • Lack of aldosterone effect (serum ↑ K+, ↓ Na+) / Deficient aldosterone (CAH) • Pseudohypoaldosteronism type I • Extra-renal Loss: Urine Na < 20 mEq/L • Gastrointestinal (emesis, diarrhea) • Skin (CF, sweating, or burns) • Third space losses (pancreatitis, burns, effusions, ascites) Hypervolemic Hyponatremia • Hypoalbuminemia due to gastrointestinal disease/ Nephrotic syndrome/ Cirrhosis • Congestive heart failure • Renal failure • Capillary leak due to sepsis
Hyponatremia- types Euvolemic Hyponatremia • Syndrome of inappropriate antidiuretic hormone • Usually ADH secreted due to ↓ vol ↑ osm. • Can be released due to pain, nausea, vomiting, morphine • Glucocorticoid deficiency • Hypothyroidism • Water intoxication – diluted formula, swimming, child abuse • Water enemas Pseudohyponatremia • Hyperglycemia • Mannitol
Hyponatremia • Clinical Presentation • Degree of symptoms depend on Na+ level and rate of decrease • Symptoms: • Anorexia • Nausea, emesis • Malaise, muscle cramps, and weakness. • Lethargy, confusion, agitation, headache, seizures, coma, decreased reflexes, hypothermia • Cheyne-Stokes respirations,
Hyponatremia- Diagnosis History can tell you most of the story Laboratory studies: Urine Na and Osm compared to Serum Na and Osm Calculate Osmolar Gap: Difference between measured & calculated osm Gap is high with mannitol, glycerol, lactate, methanol, EtOH, ethylene glycol Calc Osm= 2( Serum Na + serum K+) + (BUN/2.8) + (glucose/18)
Hyponatremia- Treatment Correction: in chronic hypo Na- correct by no more than 8-12mEq/L each day • In acute hypoNa: brain doesn’t have time to adapt. So less risk of CPM • Active CNS symptoms often improve after receiving 4–6mL/kg of 3% sodium chloride. Correction by TYPE of hyponatremia • Hypovolemic hyponatremia: replace the Na and H20 deficit • restore the intravascular volume with isotonic saline- suppresses ADH which permits excretion of the excess water. • monitoring of the sodium to avoid overly rapid correction • Hypervolemic hyponatremia: excess H20 and Na. • Don’t give Na -causes volume overload and edema. • Restrict water and sodium (2/3 maintenance) • Diuretics • Infusion of albumin if low albumin • CHF: improving cardiac output improves diuresis. • Renal failure: fluid restriction or dialysis. • Isovolemic hyponatremia: excess of water and a mild Na deficit. • Eliminate the excess water. • For acute water intoxication, give 3% Na to reverse cerebral edema. • For chronic hyponatremia from poor solute intake, give appropriate formula, and eliminate excess water
Hyponatremia- Treatment IVF replacement • 3% NS: 513 mEq/L of Na • 1ml/kg of 3% Na increases serum Na by 1.6 mEq/L • NS: 154 mEq/ L of Na • ½ NS: 77 mEq/ L of Na • ¼ NS: 38.5 mEq/ L of Na How much Na do you need to give? • Maintenance needs: Sodium: 2–3mEq/kg/24hr • Deficit Replacement: • Estimate Water = % dehydration X patient's weight • Calculated Na deficit from serum • Serum Na Deficit= [0.6 x Wt(kg)] x [Desired Na- Actual Na] • Ongoing Losses: • Diarrhea: Na content 55 mEq/L • Gastric fluids: Na content 60mEq/L • Sweat: 5–40 mEq/L of Na
Hyponatremia: Complications Physiology review: Hyponatremia= decreased plasma osmolarity (except in extreme hyperglycemia)---Water flow from low solute (low osm) to high solute (high osm)---So water flow from extracellular space into intracellular space ---Cells SWELL! Brain adapts to the decreased extracellular osmolality by decreasing its internal osmolality. Initially, through loss of sodium, potassium, and chloride. Chronically there is loss of intracellular osmoles such as amino acids. • Treatment complications: overly rapid correction • Central pontine myelinolysis • Extrapontine myelinolysis • Both = osmotic demyelination syndrome
Fun Facts 67% of cases presenting with Human Ehrlichiosis have hyponatremia … of course, they also have fever (100%), thrombocytopenia (92%), and rash (67%)
Hypernatremia Serum Na >145 mEq/L [deficit of (TBW) relative to Na] • Primarily hospital-acquired →in children who have restricted access to fluids. • Incidence >1% in hospitalized patients. CAUSES: • Water deficit • Salt Excess • Water depletion exceeding sodium depletion Sodium is unique among electrolytes… because water balance, not sodium balance, usually determines its concentration.
Hypernatremia: CausesWater Loss Water Loss/ Deficit • Renal • Central DI • Nephrogenic DI • Insensible Losses • Excessive perspiration • Fever/ Heat exhaustion/Heatstroke • Respiratory Illness • Prematurity-large surface area • large evaporative water losses • Phototherapy or radiant warmers • Inadequate Intake • Ineffective breastfeeding • Child abuse/neglect • Adipsia (lack of thirst)
Hypernatremia-Causes Water and Sodium Deficit • Gastrointestinal losses • Diarrhea • Emesis/nasogastric suction • Osmotic cathartics (lactulose) • Cutaneous losses • Burns • Excessive sweating • Renal losses • Osmotic diuretics (mannitol) • Diabetes mellitus • Chronic kidney disease (dysplasia and obstructive uropathy) • Polyuric phase of acute tubular necrosis • Postobstructive diuresis
Hypernatremia- Causes Excessive Sodium • Improperly mixed formula • Excess sodium bicarbonate • Ingestion of seawater or sodium chloride • Intentional salt poisoning • (child abuse) • Intravenous hypertonic saline • Hyperaldosteronism
Note ↓ skin turgor is a LATE sign (doughy) Irritability or lethargy High-pitched cry or wail Altered sensorium Seizures Increased muscle tone Fever Rhabdomyolysis Oligouria Severe hypernatremic dehydration induces brain shrinkage tears cerebral blood vessels→ cerebral hemorrhage venous sinus thrombosis seizures, paralysis, and encephalopathy Brain cell volume can ↓10% to 15% acutely Within 1 hour, the brain ↑ intracellular Na and K, amino acids, & idiogenic osmoles Within 1 week, the brain regains 98% of its water content. Hypernatremia: signs and symptoms In patients with prolonged hypernatremia, rapid rehydration with hypotonic fluids may cause cerebral edema, which can lead to coma, convulsions, and death.
Hypernatremia: Work-up • Serum sodium, glucose, osmolality, BUN, and creatinine levels must be measured. • Urine volume, urine osmolality and urine electrolyte levels • Assess renal concentrating ability • Quantify the urinary free water losses • urine osm (<800 mmol/L) with serum hypernatremia = renal concentrating defect • Urine tests of sodium concentration and osmolality • Hypovolemic hypernatremia • Extrarenal losses show urine sodium levels of <20 mEq/L • Renal losses urine sodium values are >20 mEq/L. • In euvolemic hypernatremia, urine sodium data vary. • In hypervolemic hypernatremia, the urine sodium level is >20 mEq/L. • Imaging studies • In alert, severely hypernatremic patients: rule out a hypothalamic lesion • affecting the thirst center. • CT /MRI scans show intracranial pathologies.
Hypernatremia: Treatment Correct fluid deficit first Rapid correction can cause cerebral edema. Dehydration should be corrected over 48-72 hours. The rate of sodium correction: 10-12 mEq/L in 24 hours. Calculation of body water deficit: In children, TBW is 60% of lean body weight. TBW = 0.6 X weight. An exception is babies, with TBW around 80% of their body weight. 1. Water deficit (L) = [(current Na mEq/L ÷ 145 mEq/L) - 1] X 0.6 X Wt (kg) or 2. Water deficit(L)= 4ml x Wt(kg) x (desired change in Na mEq/L) • Example calculation: A child weighs 10 kg with Na= 160 mEq/L. • With first equation, water deficit (L) = [(160 mEq/L ÷ 145 mEq/L) - 1] X 0.6 X 10 = 0.62 L. • With second equation, water deficit (L)= 4ml x 10 kg x 15 mEq/L Na change = 600ml= 0.6 L
Hypernatremia: treatment If acutely hypotensive, use NS or LR first to restore some volume. Avoid D5W if hyperglycemia is present
I’m not fat… I’m just really swollen from the salt in my chili cheese fries
Potassium Homeostasis • Most potassium is intracellular • Distribution of between the intra- and extracellular compartments alters serum levels • Na+, K+-ATPase maintains the high intracellular K+ concentration • Pumping Na+ out of the cell and K+ into the cell. • Insulin activates the Na+, K+-ATPase- drives K+ into the cell • Acidosis (high H+) drives potassium extracellularly; (H+ in for K+ out) • Alkalosis drives K+ into the cell • β-Adrenergic agonists stimulate the Na+, K+-ATPase, ↑cellular uptake of K+ • α-Adrenergic agonists and exercise cause a net movement of K+ out. • Potassium is necessary for: • Electrical responsiveness of nerve and muscle cells • Contractility of cardiac, skeletal, and smooth muscle.
Homeostasis- controlled by EXCRETION Kidney plays the most important role • 90% is of K+ is resorbed before the distal tubule and collecting duct- • In distal tubule and collecting duct- K+ absorbed and secreted • Tubular secretion that regulates the amount of K+ in the urine • Regulating hormone- aldosterone (↑in hyperkalemia) • Acts on cortical collecting duct • Moves sodium into cells • Creates a negative charge in the lumen → K+ excretion. • ↑ intracellular Na+ stimulates the basolateral Na+, K+-ATPase • Moves K+ into cells lining the cortical collecting duct from blood side. • Glucocorticoids, ADH, high urine flow, and high Na+ delivery to the distal nephron also ↑ urine K+. • Alkalosis -↑ urine K+. • Acidosis ↓ urine K+. • Excretion is decreased by insulin, catecholamines, and urine ammonia
Hyperkalemia- Pathophysiology “One of the few things you can die from without any symptoms…” Causes Spurious Increased Intake Decreased Excretion Transcellular shifts
Hyperkalemia- Causes • Spurious (Lab error) • Hemolysis- during heelstick, or clenched fist • Tissue ischemia- during blood drawing • Thrombocytosis/ Leukocytosis- release of K+ during clot formation • Storage of specimen in cold- causes K+ release from cells • Increased Intake • IV fluid administration/ TPN • Excess oral dosing • Blood transfusions • Transcellular Shifts • Acidosis- less with organic acids and even less with respiratory causes • Cell destruction :Rhabdomyolysis, tumor lysis, tissue necrosis, hemolysis • Hematomas/gastrointestinal bleeding • Medicines: Succinylcholine/ Digitalis/ Fluoride/ β-Adrenergic blockers • Exercise • Hyperosmolality- water flows out of cells and K+ follows (Mannitol ,etc) • Insulin deficiency • Malignant hyperthermia - muscles release K+ • Hyperkalemic periodic paralysis
Hyperkalemia- Causes • Decreased Excretion • Renal failure • 1° adrenal disease - ↓aldosterone leads to ↑K+ by decreased excretion • Acquired Addison disease- metabolic acidosis, salt wasting and hyponatremia • 21-hydroxylase deficiency 3β-hydroxysteroid dehydrogenase deficiency • Kidney damage- deficient Renin- Hyporeninemic hypoaldosteronism – • Met acidosis/Na+ ok • Urinary tract obstruction • Sickle cell disease • Kidney transplant • Lupus nephritis • Renal tubular disease- • Pseudohypoaldosteronism type I- ↑Aldosterone- Met acidosis, Salt wasting (↓Na) • Acquired tubular dysfxn (Sickle cell, lupus)- impaired H+ and K+ excretion • Medications • Angiotensin-converting enzyme inhibitors/ Angiotensin II blockers • Potassium-sparing diuretics • Nonsteroidal anti-inflammatory drugs • Trimethoprim • Heparin
Hyperkalemia CLINICAL MANIFESTATIONS. • Effects on membrane polarization. • Cardiac - (ECG) changes – • peaked T waves • ↑P-R interval • flat P wave • wide QRS • Eventually progress to ventricular fibrillation and Asystole • Skeletal Muscles/ Nerves • Paresthesias • Weakness • Tingling.
Hyperkalemia DIAGNOSIS. • Spurious hyperkalemia is very common in children, get repeat value! • Basic Metabolic Panel- renal fxn and acid-base status. • If Hyponatremia and volume depletion due to salt wasting- think low aldosterone • Phosphorus and Uric Acid • If Hyperphosphatemia and hyperuricemia- think causes of cell death • Tumor lysis syndrome • Rhabdomyolysis- Elevated creatinine phosphokinase (CPK) level and ↓Ca • Hemolysis- Hemoglobinuria and a decreasing hematocrit • When no clear etiology - differentiating decreased potassium excretion from the other etiologies • Measuring urinary potassium to assess renal excretion of potassium. • The transtubular potassium gradient (TTKG) = [K]urine/[K]plasma × (plasma osm/urine osm)urine osmolality > serum osmolality for the result to be valid. TTKG should be >10 in hyperkalemia (<8 suggests a defect in renal K+ excretion) • Aldosterone level
Hyperkalemia- Treatment K+ level, the ECG, and the risk determine the aggressiveness of therapy. • Stop all sources of additional potassium (oral, intravenous) • If K+ level is believable at >6.0 mEq/L, get EKG Stabilize the heart to prevent life-threatening arrhythmias • Calcium-stabilizes the cell membrane of heart cells Rapidly decrease serum K+ level (even if only temporary) • Bicarbonate- K+ to move intracellularly, lowering the plasma K+ level • Insulin- K+ to move intracellularly, give with glucose • Albuterol neb- stimulates β1-receptors→rapid movement of K+ into cells
Hyperkalemia- Treatment Remove potassium from the body. • Loop diuretic increases renal excretion of K+- only if making urine. • Kayexalate- exchange resin that is given either rectally or orally • Dialysis for acute potassium removal • necessary if severe renal failure or high rate of endogenous K+ release • Hemodialysis better than Peritoneal dialysis • Chronic management • reducing dietary intake and eliminating or reducing medications that cause hyperkalemia. May need meds to remove K+ • Fludrocortisone – Aldosterone deficiency states
Hypokalemia Hypokalemia in kids is common Usually associated with gastroenteritis Causes: • Decreased intake • Increased losses: extrarenal and renal • Transcellular shifts • *Lab error- spurious
Causes of Low Potassium Decreased Intake • Anorexia • Malnutrition Spurious • High white blood cell count • Cells take up extracellular K+ while waiting for specimen to be put in machine • Leukemia • High WBC from other causes
Causes of Low Potassium- Losses EXTRARENAL LOSSES • Diarrhea • Laxative abuse • Sweating • Kayexalate or clay ingestion
Causes of Low Potassium- Losses Renal Losses • Metabolic acidosis • Renal tubular acidosis (usu distal, rarely proximal) • Ureterosigmoidostomy • Diabetic ketoacidosis • Metabolic alkalosis (↑aldosterone- ↑ urine K+ and H+ excretion) • Emesis / nasogastric suction- • Gastric loss of K+ and HCL→kidney secretes HCO3→ Na + K lost too • Chloride-losing diarrhea – AR D/O with unusual met alkalosis with diarrhea • Cystic fibrosis – chloride loss in sweat • Without specific acid-base disturbance • Tubular toxins: amphotericin, cisplatin, aminoglycosides • also see Na+ and Mg++ losses • Interstitial nephritis • Diuretic phase of acute tubular necrosis, post-obstructive
Causes of Low Potassium- Losses Renal Losses- continued • High urine chloride and normal blood pressure • ↑urinary loss of K+ & Cl- with volume depletion and ↑aldosterone • Gitelman (↓urinary Ca with ↑urinary Mg) → • Bartter syndrome (↑Urinary Ca) • Loop and thiazide diuretics • High urine chloride and high blood pressure • Usually mediated by inappropriately high aldosterone levels • Adrenal adenoma or hyperplasia • (1°Hyperaldost→Na/Cl rentention→water retention and HTN) • Renal artery stenosis or Renin-secreting tumor • activates R-A-A system • 17α- or11β-hydroxylase deficiency • 11β-hydroxysteroid dehydrogenase def. • Cushing syndrome- mineralcorticoid activity of cortisol • Licorice ingestion- inhibits 11β-hydroxysteroid dehydrogenase • Liddle syndrome • (AD mutation of Aldosterone responsive Na channel- upregulated) • See low aldosterone levels
Clinical Manifestations of Hypokalemia Heart Muscle • ECG changes • flattened T wave • depressed ST segment • appearance of a U wave • Ventricular fibrillation and Torsades de pointes • Skeletal muscle include muscle weakness and cramps or paralysis • (if K <2.5 mEq/L) • Usually starts with the legs, followed by the arms. • Respiratory paralysis may require mechanical ventilation. • Rhabdomyolysis • Gastrointestinal motility is slowed • Constipation • Ileus with levels <2.5 mEq/L • Bladder dysfunction- urinary retention. • Chronic hypokalemia may cause kidney damage
Diagnosis- Hypokalemia • .Presence of hypertension suggests excess mineralocorticoids. • Electrolyte abnormalities are useful clues. • Diarrhea and RTA: hypokalemia and non-AG metabolic acidosis • Vomiting and NG losses- hypo K and met. Alkalosis • LABS: • Urinary potassium distinguishes between renal and extrarenal losses. • Urinary potassium losses • 24-hr urine • spot K+/Creat ratio • fractional excretion of K+ • Calculation: TTKG = [K]urine/[K]plasma × (plasma osm/urine osm) • The urine osmolality > serum osmolality for the result to be valid. • A TTKG of >4 in the presence of hypokalemia suggests excessive urinary losses of potassium.
Treatment- Hypokalemia Severe, symptomatic hypokalemia requires aggressive treatment Because of the risk of hyperkalemia, use IV potassium cautiously 0.5–1 mEq/kg, usually given over 1 hr. The adult maximum dose is 40 mEq. Oral potassium is safer.Potassium chloride is the usual choice for supplementation.Potassium acetate or potassium citrate for patients with acidosis and hypokalemia Potassium phosphate if hypophosphatemia is present Potassium-sparing diuretics- for patients with excessive urinary losses • If hypokalemia, metabolic alkalosis, and volume depletion are present (with gastric losses): Restore volume with NS to help decrease urinary potassium losses. • Disease-specific therapy is effective in many of the genetic tubular disorders.
Phosphorus Metabolism • Phosphate is critical for many cellular processes. • Major component of the bone, nucleic acids, ATP, acid-base buffers, and enzymes • < 1% of body phosphorus is in the plasma • The serum concentration of phosphate may not reflect true phosphate stores. • VARIES significantly with age!!!
INTAKE Phosphorus is readily available in food. (Dairy products, meat, & fish). GI absorption is proportional to intake, with 65% of intake absorbed- mostly in the small intestine. Absorption of phosphate can be blocked by aluminum-, calcium-, and magnesium-containing antacids. Stool losses can be increased in severe diarrhea or intestinal malabsorption. Bone metabolism of phosphate is affected by bone formation and destruction EXCRETION Excretion matches intake, except for the needs for growth. The kidney regulates phosphorus balance 90% of plasma phosphate is filtered at the glomerulus. A sodium-phosphate co-transporter mediates uptake at the PCT PTH =↓ renal resorption of phos Calcitriol (1,25 Vit D) ↑ intestinal absorption of phos and helps renal resorption of phos. Phosphorus Homeostasis
Hypophosphatemia • Causes • Decreased Intake • Increased excretion • Transcellular shifts
Decreased intake of phosphorus • Nutritional deficiency • Anorexia • Malnutrition • Impaired absorption (IBD, chronic diarrhea, celiac dz) • Premature infants (↑ needs compared to term infants) • Low phosphorus formula • Antacids and other phosphate binders (prevent absorption) • Renal failure treatment • Antacid overuse
Increased Excretion • Hyperparathyroidism • Parathyroid hormone–related peptide (malignancy) • Tumor-induced osteomalacia • Hypophosphatemic rickets • Fanconi syndrome • Dent disease (x-linked defective chloride channel) • Mutations in sodium-phosphate cotransporter • Volume expansion and intravenous fluids • Metabolic acidosis (phosphorus shifts out of cells then excreted by kidney) • Diuretics • Others
Transcellular Shifts Overall- increased intracellular use of phosphorus • Glucose infusioninsulin release • Insulinshift of glucose and phosphorus into cells • Refeedinganabolic state leads to ↑cellular demand for phos • Usually in first 5 days of refeeding • Total parenteral nutrition (insufficient supplementation) • Respiratory alkalosis↑intracellular pH stimulates intracellular metabolism and increased phos use • Tumor growth (leukemia/lymphoma due to ↑ use by tumors) • Bone marrow transplantation • Hungry bone syndrome (use of phos/ca/mg) after parathyroidectomy
Multifactorial • Vitamin D deficiency • impaired intestine absorption • hyperPTH causes ↑ renal phosphorus losses • Sepsis • Dialysis
Clinical Manifestations • Usually asymptomatic if mild • Severe acute hypophosphatemia • <1-1.5mg/dL • rhabdomyolysis, hemolysis, cardiac dysfunction and neurologic symptoms. • Chronic hypophosphatemia • proximal muscle weakness and atrophy • Rickets • Short stature