Download
1 / 1
10 likes | 130 Vues
Hypotension in Acute Decompensated Heart Failure: Findings from ASCEND-HF.

E N D
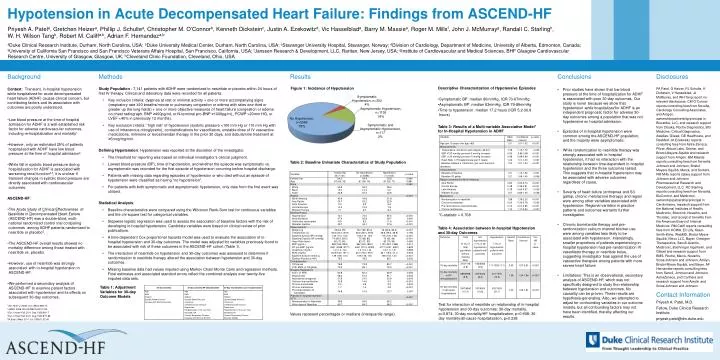
Hypotension in Acute Decompensated Heart Failure: Findings from ASCEND-HF Priyesh A. Patela, Gretchen Heizera, Phillip J. Schultea, Christopher M. O’Connorb, Kenneth Dicksteinc, Justin A. Ezekowitzd, Vic Hasselblada, Barry M. Massiee, Roger M. Millsf, John J. McMurrayg, Randall C. Starlingh, W. H. Wilson Tangh, Robert M. Califfa,b, Adrian F. Hernandeza,b aDuke Clinical Research Institute, Durham, North Carolina, USA; bDuke University Medical Center, Durham, North Carolina, USA; cStavanger University Hospital, Stavanger, Norway; dDivision of Cardiology, Department of Medicine, University of Alberta, Edmonton, Canada; eUniversity of California San Francisco and San Francisco Veterans Affairs Hospital, San Francisco, California, USA; fJanssen Research & Development, LLC, Raritan, New Jersey, USA; gInstitute of Cardiovascular and Medical Sciences, BHF Glasgow Cardiovascular Research Centre, University of Glasgow, Glasgow, UK; hCleveland Clinic Foundation, Cleveland, Ohio, USA • Conclusions • Prior studies have shown that low blood pressure at the time of hospitalization for ADHF is associated with poor 30-day outcomes. Our study is novel because we show that hypotension while hospitalized for ADHF is an independent prognostic factor for adverse 30-day outcomes among a population that was not hypotensive on hospital admission. • Episodes of in-hospital hypotension were common among the ASCEND-HF population, and the majority were asymptomatic. • While randomization to nesiritide therapy was strongly associated with in-hospital hypotension, it had no interaction with the relationship between time-dependent in-hospital hypotension and the three outcomes tested. This suggests that in-hospital hypotension may be associated with adverse outcomes regardless of cause. • Severity of heart failure (orthopnea and S3 gallop, chronic metolazone therapy) and region were among other variables associated with hypotension. Regional variation in practice patterns and outcomes warrants further investigation. • Chronic bumetanide therapy and pre-randomization calcium channel blocker use were among variables less likely to be associated with hypotension. Interestingly, smaller proportions of patients experiencing in-hospital hypotension had pre-randomization IV vasodilator therapy or nesiritide bolus, suggesting investigator bias against the use of vasoactive therapies among patients with more severe heart failure. • Limitations: This is an observational, secondary analysis of ASCEND-HF, which was not specifically designed to study the relationship between hypotension and outcomes. No causality can be proven. These results are hypothesis-generating. Also, we attempted to adjust for confounding variables in our outcome models, but all confounding factors may not have been identified, thereby affecting our results. Disclosures PA Patel, G Heizer, PJ Schulte, K Dickstein, V Hasselblad, JJ McMurray, and WH Tang report no relevant disclosures. CM O’Connor reports consulting fees from Novella, Cardiology Consulting Associates, and Amgen, ownership/partnership/principal in Biscardia, LLC, and research support from Otsuka, Roche Diagnostics, BG Medicine, Critical Diagnostics, Astellas, Gilead, GE Healthcare, and ResMed. JA Ezekowitz reports consulting fees from Astra-Zeneca, Pfizer, Abbott Labs, Servier, and Bristol-Meyers-Squibb and research support from Amgen. BM Massie reports consulting fees from Novartis, Johnson and Johnson, Bristol-Meyers-Squibb, Merck, and Sorbent. RM Mills reports salary support from Johnson and Johnson Pharmaceutical Research and Development, LLC. RC Starling reports consulting fees from Novartis, BioControl, and Medtronic, ownership/patnership/principal in Cardiomems, research support from the National Institutes of Health, Medtronic, Biotronik, Novartis, and Thoratec, and receipt of benefits from the American Board of Internal Medicine. RM Califf reports consulting fees from KOWA, Eli Lilly, Glaxo Smith-Kline, WebMD, Bristol-Myers-Squibb, Nitrox LLC, Bayer, Orexigen Therapeutics, Sanofi-Aventis, Medtronic, BoehringerIngelheim, and Gilead and research support from BMS, Roche, Merck, Novartis, Scios/Johnson and Johnson, Amilyn, Bristol-Myers-Squibb, and Bayer. AF Hernandez reports consulting fees from Sanofi, Johnson and Johnson, AstraZeneca, and Corthera and research support from Amylin and Scios/Johnson and Johnson. • Methods • Study Population : 7,141 patients with ADHF were randomized to nesiritide or placebo within 24 hours of first IV therapy. Clinical and laboratory data were recorded for all patients. • Key inclusion criteria: dyspnea at rest or minimal activity + one or more accompanying signs (respiratory rate ≥20 breaths/minute or pulmonary congestion or edema with rales one-third or greater up the lung fields) + one or more objective measures of heart failure (congestion or edema on chest radiograph, BNP ≥400pg/mL or N-terminal pro-BNP ≥1000pg/mL, PCWP >20mm HG, or LVEF <40% in previously 12 months). • Key exclusion criteria: “high risk” of hypotension (systolic pressure <100 mm Hg or 110 mm Hg with use of intravenous nitroglycerin), contraindications for vasodilators, unstable dose of IV vasoactive medications, milrinone or levosimendan therapy in the prior 30 days, and dobutamine treatment at ≥5mcg/mg/min. • Defining Hypotension: Hypotension was reported at the discretion of the investigator. • The threshold for reporting was based on individual investigator’s clinical judgment. • Lowest blood pressure (BP), time of hypotension, and whether the episode was symptomatic vs. asymptomatic was recorded for the first episode of hypotension occurring before hospital discharge. • Patients with missing data regarding episodes of hypotension or who died without an episode of hypotension were classified as having “no hypotension”. • For patients with both symptomatic and asymptomatic hypotension, only data from the first event was utilized. • Statistical Analysis: • Baseline characteristics were compared using the Wilcoxon Rank-Sum test for continuous variables and the chi-square test for categorical variables. • Stepwise logistic regression was used to assess the association of baseline factors with the risk of developing in-hospital hypotension. Candidate variables were based on clinical review of prior publications. • A time-dependent Cox proportional hazards model was used to evaluate the association of in-hospital hypotension and 30-day outcomes. The model was adjusted for variables previously found to be associated with risk of these outcomes in the ASCEND-HF cohort (Table 1). • The interaction of nesiritide on hypotension and 30-day outcomes was assessed to determine if randomization to nesiritide therapy altered the association between hypotension and 30-day outcomes. • Missing baseline data had values imputed using Markov Chain Monte Carlo and regression methods. Final estimates and associated standard errors reflect the combined analysis over twenty-five imputed data sets. Results Background Context: Transient, in-hospital hypotension while hospitalized for acute decompensated heart failure (ADHF) causes clinical concern, but contributing factors and its association with outcomes are poorly understood. • Low blood pressure at the time of hospital admission for ADHF is a well-established risk factor for adverse cardiovascular outcomes, including re-hospitalization and mortality1. • However, only an estimated 25% of patients hospitalized with ADHF have low blood pressure at the time of hospital admission2. • While fall in systolic blood pressure during hospitalization for ADHF is associated with worsening renal function3,4, it is unclear if transient changes in systolic blood pressure are directly associated with cardiovascular outcomes. ASCEND-HF: • The Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND-HF) was a double-blind, multi-national randomized control trial comparing outcomes among ADHF patients randomized to nesiritide or placebo5. • The ASCEND-HF overall results showed no mortality difference among those treated with nesiritide vs. placebo. • However, use of nesiritide was strongly associated with in-hospital hypotension in ASCEND-HF. • We performed a secondary analysis of ASCEND-HF to examine patient factors associated with hypotension and its effects on subsequent 30-day outcomes. Descriptive Characterization of Hypotensive Episodes • Symptomatic BP: median 80mmHg, IQR 70-87mmHg • Asymptomatic BP: median 83mmHg, IQR 79-88mmHg • Time to hypotension: median 17.2 hours (IQR 5.2-30.8 hours) Table 3: Results of a Multi-variable Associative Model* for In-Hospital Hypotension in ADHF Table 2: Baseline Univariate Characteristics of Study Population *C-statistic = 0.708 Table 4: Association between In-hospital Hypotension and 30-day Outcomes Table 1: Adjustment Variables for 30-day Outcome Models Contact Information Priyesh A. Patel, M.D. Fellow, Duke Clinical Research Institute priyesh.patel@dm.duke.edu Test for interaction of nesiritide on relationship of in-hospital hypotension and 30-day outcomes: 30-day mortality, p=0.874; 30-day mortality/HF hospitalization, p=0.908; 30-day mortality/all-cause hospitalization, p=0.238 1Am Heart J. 2008. Oct;156(4):662-73. 2JAMA. 2006. Nov 8;296(18):2217-26. 3Eur J Heart Fail. 2011 Sep;13(9):961-7. 4Eur J Heart Fail..2011 Aug;13(8):877-84. 5N Engl J Med. 2011 Jul 7;365(1):32-43. Values represent percentages or medians (interquartile range).