Download
1 / 24
250 likes | 535 Vues
Chronic Venous Disease. Patrik Tosenovsky. Issues. Severity of CVD Appropriate referral Benefit, side effects and cost of the treatment. CVD – Chronic Venous Disorders. Include s spectrum of clinical presentations ranging from teleangiectasias to venous ulceration.

E N D
Chronic Venous Disease Patrik Tosenovsky
Issues • Severity of CVD • Appropriate referral • Benefit, side effects and cost of the treatment
CVD – Chronic Venous Disorders • Include s spectrum of clinical presentations ranging from teleangiectasias to venous ulceration. • Primary vs Secondary
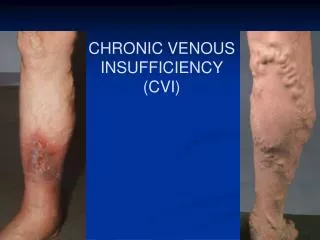
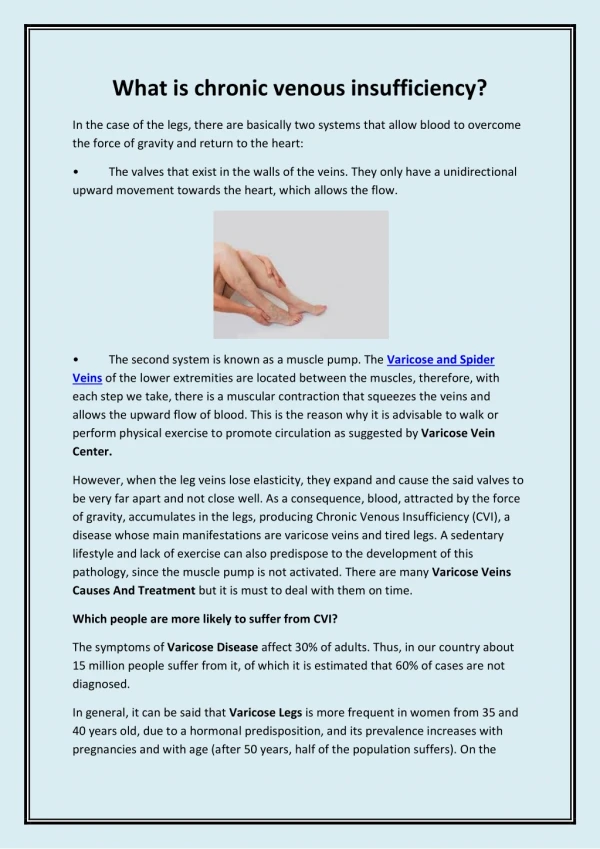
Chronic Venous Insufficiency • Usually refers more specifically to the spectrum of skin changes associated with venous hypertension
Primary CVD vs Secondary CVD • Primary - The cause is unknown (varicose veins etc) --- varicose veins/swelling/skin changes • Secondary – usually following DVT --- obstruction +/- reflux ---venous hypertension --- varicose veins/swelling/skin changes
Obstruction – Reflux – or both REFLUX or OBSTRUCTION or both OBSTRUCTION
Competent valve and obstruction free lumen is the key for function
Classification of CVD • CEAP classification • C – Clinical signs (1-6 i.e. retic.v.- ulcer) • E – ethiology (cong., primary, second.) • A – anatomy (deep, perf., superf) • P – pathophysiology (reflux, obstruction, both)
Severity of CVD • Venous Clinical Severity Score (VCSS) – more for research purposes and databases • Clinically more practical: • Active ulcer, previous ulcer, lipodermatosclerosis • Symptomatic - any stage of CVD • Other (incl. vv’s, spider veins etc)
Severity of Acute venous disease • DVT – 2 weeks of duration • Severity: • Iliofemoral DVT + swelling/discoloration • Other DVT (femoropopliteal, tibial, gastrocn., soleus veins)
Treatment options • Non-surgical – compression (venous hypertension) • Sclerotherapy – both for cosmetic vv’s and synptomatic ones • Surgical – phlebectomy/stripping • Percutaneous – RFA, Laser, angioplasty/stent • Deep vein reconstruction • Combined
How effective is the treatment • Percutaenous and open surgical – up to 98% success rate (no difference) • Sclerotherapy – good for small veins • Angioplasty – up to 99% success rate for iliac veins • Deep vein reconstruction – 60 % success
Venous ulcers healed 12th week post deep vein reconstruction