Download
1 / 37
440 likes | 1.04k Vues
The Global Burden of Disease. The scale of the problem. Leading Causes of Death and Disability (DALY’s). 1990. 2020. Rank Cause % Rank Cause %. 1 Lower respiratory infections 8.2 1 Ischemic heart disease 5.9 2 Diarrhoeal diseases 7.2 2 Major depression 5.7

E N D
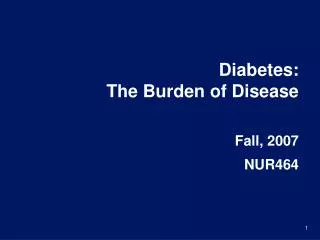
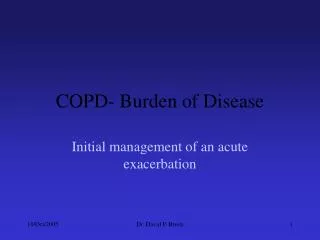
The Global Burden of Disease The scale of the problem
Leading Causes of Death and Disability (DALY’s) 1990 2020 Rank Cause % Rank Cause % 1 Lower respiratory infections 8.2 1 Ischemic heart disease 5.9 2 Diarrhoeal diseases 7.2 2 Major depression 5.7 3 Perinatal conditions 6.7 3 Road traffic accidents 5.1 4 Major depression 3.7 4 Cerebrovascular disease 4.4 5 Ischemic heart disease 3.4 5 COPD 4.2 6 Cerebrovascular disease 2.8 6 Lower respiratory infections 3.1 7 Tuberculosis 2.8 7 Tuberculosis 3.0 8 Measles 2.7 8 War 3.0 9 Road traffic accidents 2.5 9 Diarrhoeal diseases 2.7 10 Congenital abnormalities 2.4 10 HIV 2.6 Global Burden of Disease Study, 1996
* * * * Mortality due to leading global risk factors World Health Report 2002
Prevalence of ‘Hypertension’ by different cut points 90 = 25.3% 95 = 14.5% 100 = 8.4% 105 = 4.7% % of screened population 110 = 2.9% 115 = 1.4% 50 60 70 80 90 100 110 120 130 Diastolic BP, mmHg
British Hypertension Society Guidelines for hypertension management 2004 (BHS-IV): summary Bryan Williams, Neil R Poulter, Morris J Brown, Mark Davies, Gordon T McInnes, John F Potter, Peter S Sever, Simon McG Thom; the BHS guidelines working party, for the British Hypertension Society BMJ Volume 328 13 March 2004 634-640.
BHS Guidelines • Definitions • Measurement • Risk assessment • Evaluation of hypertensive patients • Thresholds for intervention • Treatment goals • Lifestyle measures • Choice of therapy • Meta-analysis of trials • ABCD rule • Aspirin and statins • Follow up and implementation
Classification of blood pressure levels of the British Hypertension Society
Blood pressure measurement by standard mercury sphygmomanometer or semiautomated device • Use of properly maintain, calibrated, and validated device • Measure sitting blood pressure routinely: standing blood pressure should be recorded at least at the initial estimation in elderly or diabetic patients • Remove tight clothing, support arm at heart level, ensure arm relaxed and avoid talking during the measurement procedure • Use of cuff of appropriate size Continued
Blood pressure measurement by standard mercury sphygmomanometer or semiautomated device • Lower mercury column slowly (2mm per second) • Read blood pressure to the nearest 2 mm Hg • Measure diastolic blood pressure as disappearance of sounds (phase V) • Take the mean of at least two readings, more recordings are needed if marked differences between initial measurements are found • Do not treat on the basis of an isolated reading
Potential indications for the use of ambulatory blood pressure monitoring • Unusual variability of blood pressure • Possible white coat hypertension • Informing equivocal treatment decisions • Evaluation of nocturnal hypertension • Evaluation of drug resistant hypertension • Determining the efficacy of drug treatment over 24 hours • Diagnosis and treatment of hypertension in pregnancy • Evaluation of symptomatic hypotension
Lifestyle measures • Maintain normal weight for adults (body mass index 20-25kg/m2) • Reduce salt intake to < 100mmol/day (<6g NaCI or < 2.4 g Na+/day) • Limit alcohol consumption to < 3 units/day for men and < 2 units/day for women) • Regular physical exercise (brisk walking rather than weightlifting) for > 30 minutes per day, ideally on most days of the week but at least on three days of the week. • Consume at least five portions/day of fresh fruit and vegetables • Reduce the intake of total and saturated fat
Thresholds and treatment for antihypertensive drug treatment • Drug treatment should be started in all patients with sustained systolic blood pressures > 160mmHg or sustained diastolic blood pressures > 100mmHg despite non-pharmacological measures (A) • Drug treatment is also indicated in patients with sustained systolic blood pressures 140-159mmHg or diastolic blood pressures 90-99mmHg if target organ damage is present, or there is evidence of established cardiovascular disease or diabetes, or if there is a 10 year cardiovascular disease risk of > 20% (B) continued
Thresholds and treatment for antihypertensive drug treatment • For most patients a target of < 140mmHg systolic blood pressure and <85mmHg diastolic blood pressure recommended (B). For patients with diabetes, renal impairment or established cardiovascular disease a lower target of < 130/80mmHg is recommended
Initial Blood Pressure 130-139 80-89 160-179 100-109 140-159 90-99 180/110 <130/85 160/100 140-159 90-99 <140/90 Treat Re-measure in 5 years Reassess Yearly Treat SEE NEXT SLIDE
140-159 90-99 Target organ damage or CVS complications or Diabetes or CV event risk 2%/year [>20% over 10 yrs ] No target organ damage and No CVS complications and No diabetes and CV event risk < 2%/year [<20% over 10 yrs ] Observe Reassess CV risk yearly Treat
Drug treatment of hypertension Diuretic ACE-inhibitor Most hypertensives will need 2 drugs to control BP Drug combinations may be synergistic Angiotensin receptor blocker Calcium-channel blocker Beta-blocker (Alpha-blocker)
STROKEComparisons of different active treatments BP difference (mm Hg) Favours second listed Favours first listed RR (95% CI) 2/0 ACE vs. D/BB 1.09 (1.00,1.18) 1/0 CA vs. D/BB 0.93 (0.86,1.01) 1/1 ACE vs. CA 1.12 (1.01,1.25) 0.5 1.0 2.0 Relative Risk
CORONARY HEART DISEASEComparisons of different active treatments BP difference (mm Hg) Favours first listed Favours second listed RR (95% CI) 2/0 ACE vs. D/BB 0.98 (0.91,1.05) 1/0 CA vs. D/BB 1.01 (0.94,1.08) 1/1 ACE vs. CA 0.96 (0.88,1.05) 0.5 1.0 2.0 Relative Risk
HEART FAILUREComparisons of different active treatments BP difference (mm Hg) Favours first listed Favours second listed RR (95% CI) 2/0 ACE vs. D/BB 1.07 (0.96,1.19) 1/0 1.33 (1.21,1.47) CA vs. D/BB 1/1 ACE vs. CA 0.82 (0.73,0.92) 0.5 1.0 2.0 Relative Risk
MAJOR CARDIOVASCULAR EVENTSComparisons of different active treatments BP difference (mm Hg) Favours first listed Favours second listed RR (95% CI) 2/0 ACE vs. D/BB 1.02 (0.98,1.07) 1/0 1.04 (0.99,1.08) CA vs. D/BB ACE vs. CA 1/1 0.97 (0.92,1.03) 0.5 1.0 2.0 Relative Risk
ALLHAT Design Amlodipine Chlorthalidone Doxazosin Lisinopril High risk Hypertensive Patients 42,515 Randomize 10,362 eligible for Lipid lowering Not eligible for Lipid lowering Randomize Study completion January 2003 Pravastatin Usual Care
ALLHAT Primary Endpoint: CHD Death and Nonfatal MI Relative Risk (95% CI) Amlodipine 0.98 (0.90-1.07) Lisinopril 0.99 (0.91-1.08) 0.7 1.3 Favors AmlodipineFavors Lisinopril FavorsChlorthalidone ALLHAT Collaborative Research Group. JAMA. 2002;288:2981-2997.
ASCOT: PROBE Design Amlodipine Perindopril Doxazosin GITs 19342 High-risk Hypertensive Randomized Atenolol Bendrofluazide Doxazosin GITs Eligible for Lipid Lowering Not Eligible for Lipid Lowering 10305 Randomize DB Atorvastatin 10 mg Placebo Expected Mean Follow-up: 5 Yrs Fatal CHD + Non-Fatal MI
Atorvastatin 10 mg Number of events 100 Placebo Number of events 154 36% reduction HR = 0.64 (0.50-0.83) p=0.0005 ASCOT study: Effect of atorvastatin on CHD
Atorvastatin 10 mg Number of events 89 Placebo Number of events 121 27% rreduction HR = 0.73 (0.56-0.96) p=0.0236 ASCOT study: Effect of atorvastatin on stroke
The British Hypertension Society recommendations for combining Blood Pressure Lowering drugs Younger (e.g.<55yr)and Non-Black Older (e.g.55yr) or Black Step 1 A (or B*) C or D Step 2 A (or B*) + C or D Step 3 A (or B*) + C + D Step 4Resistant Hypertension Add: either -blocker or spironolactone or other diuretic A: ACE Inhibitor or angiotensin receptor blocker B: b - blockerC: Calcium Channel Blocker D: Diuretic (thiazide) * Combination therapy involving B and D may induce more new onset diabetes compared with other combination therapies Adapted from: ‘Better blood pressure control: how to combine drugs’Journal of Human Hypertension (2003) 17, 8186
Compelling and possible indications, contraindications, and cautions for the major classes of antihypertensive drugs
USA1 27% England2 Scotland4 Canada3 6% 17.5% 16% % of hypertensives withcontrolled BP <160/95 mm Hg <140/90 mm Hg Finland4 Spain4 Australia4 19% 20% 20.5% India4 Zaire4 2.5% 9% Adapted from Mancia, 1997
Other medication for hypertensive patients • Primary prevention • Aspirin: use 75mg daily if patient is aged >50 years with blood pressure controlled to <150/90mmHg and; target organ damage, diabetes mellitus, or 10 year risk of cardiovascular disease of >20% (measured by using the new Joint British Societies cardiovascular disease risk chart) • Statin: use sufficient doses to reach targets if patient aged up to at least 80 years, with a 10 year risk of cardiovascular disease of >20% (measured by using the new Joint British Societies risk chart) and with total cholesterol concentration >3.5mmol/l • Vitamins – no benefit shown, do not prescribe
Secondary prevention (including patients with type 2 diabetes) • Aspirin:use for all patients contraindicated • Statin: use sufficient doses to reach targets if patient is aged up to at least 80 years with a total cholesterol concentration >3.5mmol/l • Vitamins – no benefits shown, do not prescribe
Age- and gender adjusted hypertension control by country (35-64 years); 140/90 mmHg
Age- and gender adjusted hypertension control by country (35-64 years); 140/90 mmHg Impact of structured algorithm