Download
1 / 53
540 likes | 649 Vues
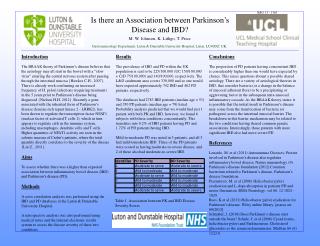
How to find an association between a disease and a gene?. Alex V. Postma Department of Anatomy, Embryology & Phsyiology Heart Failure Research Center AMC a.v.postma@amc.uva.nl. 50% of cardiac mortality US: ~250.000 SCD / year NL: ~300 SCD / week, 15.000 / year VF most common underlying

E N D
How to find an association between a disease and a gene? Alex V. PostmaDepartment of Anatomy, Embryology & PhsyiologyHeart Failure Research CenterAMCa.v.postma@amc.uva.nl
50% of cardiac mortality US: ~250.000 SCD / year NL: ~300 SCD / week, 15.000 / year VF most common underlying arrhythmia Sudden cardiac death, the numbers
> 40 y 1/1.000/year > 85% coronary artery disease < 40 y 0,8-1,6/100.000/year ~75% genetic disease Cardiomyopathies, primary electrical disease Sudden cardiac death, the causes
Monogenic Cardiac Arrhythmia Syndromes Long QT Syndrome Brugada Syndrome Catecholamine-induced PMVT/VF Short QT Syndrome Isolated Cardiac Conduction Disorders Familial Atrial Fibrillation Sinus Node Disease
LQTS, SQTS LQTS, SQTS Sinus Node Dysfunction LQTS, SQTS LQTS BrS CD AF
GENE DISORDER KCNQ1 LQTS, SQTS, AF KCNH2 LQTS, SQTS KCNE1 LQTS KCNE2 LQTS KCNJ2 LQTS, SQTS KCNA5 AF SCN5A LQTS, BrS, CD, SSS SCN4B LQTS RYR2 CPVT CASQ2 CPVT CACNA1C LQTS HCN4 SSS GJA5 AF CAV3 LQTS ANKB LQTS GPD1L BrS
From patient to genotype Patient goes to cardiologist (complaints, family history,...) Genetic counseling DNA isolated Mutation screening (PCR, sequencing) Clinical geneticist and cardiologist discuss result / treatment with patient Family screening OR Research
Where to start? Linkage analysis Screen candidate genes Perform exome / genome sequencing
Identifying genetic cause for a disease Many human diseases/phenotypes are affected by single genes. Examples include: Brown eyes (dominant to blue eyes); Ability to curl or roll up tongue (dominant to inability) PEDIGREES of large families can help identify whether a genetic disease is caused by a dominant or a recessive allele, and whether the disease is sex-linked or autosomal.
Autosomal Recessive Transmission Appears in both male and female children of unaffected parents. e.g. KCNQ1 mutations associated with Jervell Lange Nielsen Syndrome
Autosomal Recessive Transmission Appears in both male and female children of unaffected parents.
Mutation Arising De Novo e.g. Timothy Syndrome (CACNAIC)
Mutation Arising De Novo e.g. Timothy Syndrome (CACNAIC)
Compound heterozygosity (multiple variants together) Bezzina et al., Circ Res, 2003
Linkage analysis Technique to find causative regions / genes for a genetic disease Linkage is co-segregation between a disease and a set of markers >> identify regions that are consistently shared by affected relatives
Genetic markers: • Genetic markers are DNA sequences that show variations in size or sequence in the population • Occur random all over the genome off all species • Probably errors of DNA copying • Inherited to next generations Markers
Crossover has taken place Cross-over Parents A a a a b b B b Affected First generation a a A a b B b b Affected Second generation a a A a a a A a b b b b B B b b ? Affected Affected
Candidate gene approach • Study literature, study disease, hypothesize • Perform linkage analysis (on all candidate genes) • Positive linkage -> look for interesting areas of the gene • Sequence • -Find mutation….
Mutations Mutations are heritable changes in genes or chromosomes. Most mutations are SINGLE-GENE MUTATIONS that arise from errors in replication or from unrepaired damage to DNA molecules.
Types of mutations Original DNA strand Substitution Deletion Insertion
Effect on the protein Silent Missense Nonsense Frameshift Ser Thr Pro
Why mutation screening? Diagnostic screening: Confirmation clinical diagnosis (Prenatal) counseling Research: Genotype-phenotype relationship Pathophysiological mechanisms Presymptomatic screening/therapy
Not every novel change leads to disease. Interpret in conjunction with: Inheritance pattern Mechanism of disease Amino acid conservation Cis vs. trans Population/Haplotype information Structural and functional domains Mutation Interpretation
How to find a mutation DNA isolation from:
How to find a mutation The Invention of PCR Invented by Kary Mullis in 1983 First published account appeared in 1985 Awarded Nobel Prize for Chemistry in 1993
Intron-exon structure of a gene Start (ATG) Stop (TAA, TAG or TGA) 5’ 3’ AG GT PCR fragments
What is the Polymerase Chain Reaction? • A means of selectively amplifying a particular segment of DNA • The segment may represent a small part of a large complex mixture of DNAs: e.g. a specific exon of a gene • It can amplify a usable amount of DNA (visible by gel electrophoresis) in ~ 2 hours • It can amplify a single DNA molecule (e.g. from a single sperm) • PCR product usually undergoes post-PCR analysis: restriction digestion, sequencing, cloning etc
Sanger sequencing - DNA fragments are separated by size by gel electrophoresis - From the gel, the DNA sequence can be determined - Can produce DNA fragments 700-900bp long, but low throughput - The Human Genome Project used Sanger sequencing, completion took over 10 years
wildtype A I-1 ATC CRC ATA ATC CAC ATA I H I I H/R I ?
Next Generation Sequencing (NGS) a.k.a. Whole Genome/Exome Sequencing Mega Sequencing 2nd Generation Sequencing Massive parallel Sequencing High Throughput Sequencing Deep Sequencing General characteristics include: - Amplification of genetic material by PCR - Ligation of amplified material to a solid surface - Short reads applications; sequence and then use computers to assemble the small pieces
However... 20K variants identified per exome ~45% missense, 150 nonsense 150-250 unique variants / individual ETHICAL ISSUES!!!
Monogenic vs. polygenic Monogenic disease • Severe phenotype • Early onset • Rare • Mendelian inheritance Cause: Mutations (<1%) Polygenic (complex) disease • Mild phenotype • Late onset • Common • Complex inheritance Polymorphisms (>1%) Many polymorphisms with each a small effect, combined with environmental factors, explain inter-individual differences in risk
The ultimate clinical presentation not only depends on the gene affected or the type / location of the mutation but also on the GENETIC BACKGROUND on which it occurs. Clinical presentation = effect of mutation + genetic variation in genes (polymorphisms) encoding other players in that particular biological pathway Genetic modifiers
Polymorphisms ~1/300 bp is polymorphic in a population (3 million loci = 0.1% of the genome) ~1/1200 bp will differ between 2 random subjects Single Nucleotide Polymorphisms (SNPs) are the most common variants
What is the evidence for a role of polymorphisms in susceptibility to sudden cardiac death ? 1. Variability in clinical severity among patients with primary electrical disease 2. Heritability of various ECG parameters 3. Family history
Large family with SCN5A 1795insD mutation Carriers Non - carriers Total: Total: 114 114 118 118 HR ( HR ( bpm bpm ): ): 65.4 65.4 ± ± 16.8 16.8 72.0 72.0 ± ± 12.1 12.1 PQ (s): PQ (s): 0.20 0.20 ± ± 0.02 0.02 0.16 0.16 ± ± 0.03 # 0.03 # QRS (ms): QRS (ms): 115 115 ± ± 15 15 93 93 ± ± 13 # 13 # QTc QTc (s): (s): 0.48 0.48 ± ± 0.09 0.09 0.40 0.40 ± ± 0.03 # 0.03 # ST ST - - elev elev V1 V1 - - V3: V3: 21/43 (49%) 21/43 (49%) 3/36 (8%) # 3/36 (8%) # Total family members : 232 ST ST - - elev elev (mm): (mm): 1.6 1.6 ± ± 1.0 1.0 0.5 0.5 ± ± 0.6 # 0.6 # Unexplained SCD : 26 Nocturnal : 17 < 20/26 SCD 40 yr : Bezzina et al., Circ Res 1999;85:1206 van den Berg et. al. JCE. 2001;12:630-6
Reduced penetrance and variable disease expressivity and severity in patients with SCN5A 1795insD
What is the evidence for a role of polymorphisms in susceptibility to sudden cardiac death ? 1. Variability in clinical severity among patients with primary electrical disease 2. Heritability of various ECG parameters 3. Family history
Common sodium channel promoter haplotype in Asian subjects underlies variability in cardiac conduction T T T --- G C C C G ins C T C T T --- C C Frequency HaplotypeA 75.5% HaplotypeB 24% HaplotypeC 0.5% -835insGC T-1418C T-1062C G-354C T-847G C287T promoter intron1 exon 1 (non-coding) -2000 bp -1000 0 1000 Bezzina et al., Circulation 2006;113:338-44.
350 300 250 PR (msec) 200 150 100 Haplotype B is associated with slower conduction; Haplotype pair effects on PR-interval Non-Brugada syndrome controls Brugada syndrome baseline ** * ** * BB (5) AB (20) AA (45) BB (8) AB (33) AA (60) *P<0.05; **P≤0.001 Bonferroni-corrected significance level: 0.002
CHO cells Cardiomyocytes n=13, p=0.04 n=9, p=0.006 18 15 12 Fold activity 9 6 3 0 Hap A Hap B Hap A Hap B Reporter activity is reduced for Haplotype B ?
What is the evidence for a role of polymorphisms in susceptibility to sudden cardiac death ? 1. Variability in clinical severity among patients with primary electrical disease 2. Heritability of various ECG parameters 3. Family history
Family history of sudden death is an important predictor of ventricular fibrillation risk in myocardial infarction MI + VF (cases) versus MI - VF (controls) Dekker et al., Circulation 2006; 114: 1140 - 1145
ASSOCIATION STUDIES How to find the polymorphisms that confer susceptibility to sudden cardiac death? • Large sample sizes • Strict definition of clinical phenotype > same • pathophysiological mechanism
Identification of genetic determinants of SCD risk Association studies in disease populations with the SCD phenotype Identification of genetic variation associated with specific endophenotyes genetic variation SCD phenotype genetic variation SCD phenotype conduction (QRS duration) repolarization (QT interval) intermediate phenotypes (endophenotypes) - accurate measurement in large sample sizes - quantitative traits; more powerful for genetic analysis
Prolonged QT interval and risk of sudden death in the population Straus et al.,JACC 2006