Download
1 / 43
500 likes | 930 Vues
Interchangeability and study design. Drs. Jan Welink. Training workshop: Assessment of Interchangeable Multisource Medicines, Kenya, August 2009. Guidance documents. http://apps.who.int/prequal/ * Note to applicants on the choice of comparator products for the prequalification project

E N D
Interchangeability and study design Drs. Jan Welink Training workshop: Assessment of Interchangeable Multisource Medicines, Kenya, August 2009
Guidance documents http://apps.who.int/prequal/ * Note to applicants on the choice of comparator products for the prequalification project * Guideline on generics - Annex 7 (Multisource (generic) pharm. products: guidelines on registration requirements to establish interchangeability) - Annex 11 (Guidance on the selection of comparator pharm. products for equivalence assessment of interchangeable multisource (generic) products)
Regulatory Authority Mission “Assure that SAFE and EFFECTIVE drugs are marketed in the country and are available to the people”
Bioavailability Bioavailability Bioavailability means the rate and extent to which the active substance or therapeutic moiety is absorbed from a pharmaceutical form and becomes available at the site of action. plasma
Bioavailability relative bioavailability interactions absolute bioequivalence food-effect different formulations
Bioequivalence Bioequivalence: Two medicinal products are bioequivalents if they are pharmaceutical equivalents or alternatives and if their bioavailabilities (rate and extent) after administration in the same molar dose are similar to such degree that their effects, with respect to both efficacy and safety, will be essential the same.
Bioequivalence Bioavailability Pharmaceutical equivalent Pharmaceutical alternatives Bioequivalence
Bioequivalence Pharmaceutical Equivalent Products Reference Test Possible Differences Drug particle size, .. Excipients Manufacturing process Equipment Site of manufacture Batch size …. Documented Bioequivalence = Therapeutic Equivalence (Note: Generally, same dissolution specifications)
Bioequivalence Therapeutic equivalence of a multiscource product can be assured when the multiscource product is both pharmaceutically equivalent/alternative and bioequivalent. Concept of interchangeability includes the equivalence of the dosage form as well as for the indications and instructions for use.
Bioequivalence Pharmaceutical equivalent does not necessarily imply therapeutic equivalence: - difference excipients - difference manufacturing process - other variables drug performance?
Bioequivalence Therapeutic equivalent does not necessarily imply bioequivalence: - sensitivity - different formulations (IR/CR) - different active substance equivalence?
Bioequivalence pharmaceutical equivalence method: in principle comparative pharmacokinetics (AUC, Cmax) acceptance criteria: comparative rate and extent of absorption
Bioequivalence BA and BE are generally required for approvals of innovator and generic (multiscource) products. BE based on blood level determination of Cmax and AUC has become the most commonly used and successful biomarker for safety and efficacy of the drug product. BE products can be substituted for each other without any adjustment in dose or other additional therapeutic monitoring.
Bioequivalence BRIDGING STUDIES variations scale up clinical batch comm.batch changed batch innovator ref. ref. test test acceptance variations approval innovator approval generic acceptance variations ref. test test ref. test bioequiv.batch comm. batch changed batch generic scale up variations
Bioequivalence Studies necessary for : • Oral Immediate Release products • In general • Critical use medicines/Narrow therapeutic range drug products • Documented BA or BE problems related to API • Scientific evidence suggesting polymorphs of API, excipients, and/or process affecting BA • Non-oral, non-parenteral products designed to act systemically • Oral Modified Release products • Fixed-combination products with systemic absorption where at least one of the API requires an in vivo study
Bioequivalence Cases when pharmaceutical equivalence is enough: • Aqueous solutions • Intravenous solutions • Intramuscular, subcutaneous solutions • Oral solutions • Otic or ophthalmic solutions • Topical products prepared as solutions • Aqueous solution for nebulizer inhalation or nasal sprays • Powders for reconstitution as solution • Gases
Studies Different approach for establishing equivalence PD studies clinical studies in vitro methods ONLY IN EXCEPTIONAL CASE !!
Bioequivalence Important PK parameters Cmax: the observed maximum concentration of a drug measure of the rate of absorption AUC: area underthe concentration-time curve measure of the extent of absorption tmax: time at which Cmax is observed measure of the rate of absorption
Plasma concentration time profile Cmax AUC Tmax time
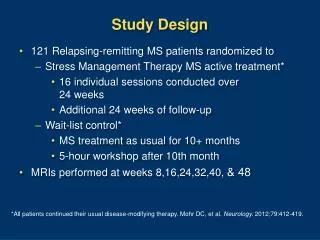
Bioequivalence – single dose Basic design considerations: minimize variability not attributable to formulations minimize bias goal: compare performance 2 formulations
Bioequivalence – single dose Golden standard study design: single dose, two-period, crossover healthy volunteers Reference (comparator)/ Test (generic)
Bioequivalence – single dose Single dose, two-period crossover: • Subjects receive in Period I and II Test/Reference Subjects: • Healthy volunteers • randomisation • Inclusion/exclusion criteria • Number of subjects
Bioequivalence – single dose • Number of subjects!! - Sample size calculation: e.g. Eur J Drug Metab Pharmacokinet 30 (2005) 41
Bioequivalence – fast/fed Administration of Test/Reference: • Normally fasted state • overnight fast • drug administration ca. 240 ml water If the SPC of the reference product contains specific recommendations in relation with food intake related to food interaction effects the study should be designed accordingly
Bioequivalence – fast/fed no change in absorption: delay in absorption: increase in absorption: decrease in absorption: Food effect:
Bioequivalence – fast/fed • If the recommendation of food intake is based onpharmacokinetic propertiessuch as higher bioavailability, then a bioequivalence study under fed conditions is generally required • If the recommendation of food intake is intended todecrease adverse events or to improve tolerability, a bioequivalence study under fasting conditions is considered acceptable although it would be advisable to perform the study under fed conditions. • If the SPC leaves a choice between fasting and fed conditions, then bioequivalence shouldpreferably be tested under fasting conditionsas this situation will be more sensitive to differences in pharmacokinetics.
Bioequivalence – fast/fed In general: follow SPC.
Sampling Blood sampling: Number of samples. Sampling times (Cmax!). knowledge drug substance Time of sampling (extrapolated AUC max. 20%). Washout phase long enough.
Bioequivalence – multiple dose Multiple dose: More relevant clinically? Less sensitive to formulation differences!
Bioequivalence – multiple dose Analytical assay sensitivity Multiple dose studies in case of….. Drug too potent/toxic for healthy volunteers –patients/ no interruption therapy Extended/modified release formulations – accumulation / unexpected behavior Non-linear PK at steady state
Bioequivalence – parallel design Crossover design preferred: - intra-subject comparison - lower variability - fewer subjects required Crossover: Parallel: R R T
Bioequivalence – parallel design Parallel design may be useful: • Drug with very long elimination half-life • Crossover design not practical Parallel design considerations: • Number of subjects • Adequate sample collection • Complete absorption • 72 hours sufficient in general
Bioequivalence – replicate vs. non-replicate Standard approach BE study: non-replicate single administration R and T average bioequivalence
Bioequivalence – replicate vs. non-replicate Replicate (RRTT or RRT or TTR): T and/or R administered twice Intra-subject variability Subject X formulation interaction average bioequivalence/ individual bioequivalence
Bioequivalence – replicate design Comparison within-subject variances T and R Indicate whether T exhibits lower or higher within-subject variability More information (performance/S*F interaction) Reduce number of subjects Scientific advantages:
Bioequivalence – replicate design Bigger commitment volunteers More administrations per subject More expensive Disadvantages:
Bioequivalence Most submitted bioequivalence studies are: Single dose studies. Fasted conditions. depends on drug substance! Crossover design. Non replicate.