Download
1 / 26
290 likes | 390 Vues
ARTHRITIS. Anna Jaatinen Rotary Doctor Bank Finland, Ilembula Hospital. Today’s topics. Osteoarthritis Rheumatoid arthritis Reactive arthritis Crystal-induced Synovitis Infectious Arthritis HIV-associated arthritis. Rheumatoid arthritis 1. Systemic diseace Unknown etiology

E N D
ARTHRITIS Anna Jaatinen Rotary Doctor Bank Finland, Ilembula Hospital
Today’s topics • Osteoarthritis • Rheumatoid arthritis • Reactive arthritis • Crystal-induced Synovitis • Infectious Arthritis • HIV-associated arthritis
Rheumatoid arthritis 1 • Systemic diseace • Unknown etiology • Symmetric inflammatory polyarthritis • Extra-articular manifestations • Rheumatoid nodules • Pulmonary fibrosis • Serositis • Vasculitis • Rheumatoid factor up to 80%
Rheumatoid arthritis 2 • Clinical Presentation • Insidous oncet of the pain, swelling and morning stiffness in the joints (hands, wrists) • Synovitis! Typical places: MCP, PIP, wrist • Rheumatoid nodules on extensor surfaces • Course is often chronic and progressive • Erosions! • Rheumatoid arthritis may substatial long-term disability and is associated with increased mortality!
Rheumatoid arthritis 3 • American Collece of Rheumatology 1987 Classification Criteria • Morning stiffness (>60 min) • Arthritis of three of more joints • Arthritis of hand joints • Rheumatoid nodules • Serum rheumatoid factor • X-ray changes (erosions and decalcification) • 4 of the 7 criteria should be met, with criteria 1 to 4 present for more than 6 weeks
Rheumatoid arthritis 4 TREATMENT • NSAID • Ibuprofen 400-800 mg TDS as long as needed • Acetylsalicylic acid • Corticosteroids • Prednison 5 to 20 mg OD • With long treatments remember to decrease the dose slowly! • Intra-articulr administration • Hydrocortison 25-100 mg i.a. • DMARDs (Diseace-modifying antirheumatic drugs) • Methotrexate • Hydroxychloroquine • Sulfasalazine • Leflunomide • Biologic DMARDs Patients with itractable symptoms may require special treatment at spesialist centre!
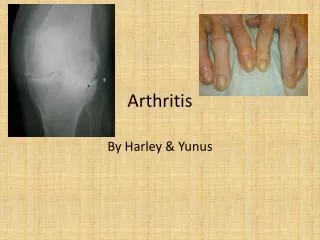
Osteoarthritis 1 = Degenerative joint disease = Arthrosis • Most common form of arthritis! • Degenerative loss of articular cartilage with subsequent formation of reactive new bone at the cartilage surface • Most common: PIP, DIP, hips, knees, cervical and lumbar spine • Common in the elderly, but may occur any age especially after joint trauma, chronic inflammatory arthritis or congenital malformation.
Osteoarthritis 2 • Clinical Presentation • Pain! • Specific clinical features depend on the joint involved • Knee: possible hydrops, no signs of infection or severe inflammation • DIP: enlarged joint Bouchard’s nodes • X-ray shows cartilage damage and sometimes even deformity
Osteoarthritis 3 TREATMENT • Nonpharmacologic approaches • Prief period of rest • Good shoes: Walkers • Crepe bandage or brace can help • Physiotherapy and exercise to affected joints • Reduction on weight in obese patients • Medications • Paracetamol 1 g TID (QID) • NSAID (As low dose as possible) • Ibuprofen 200-600 mg TID • Itra-articular clucocorticoid • Should not be given more than every 3 to 6 months • Systemic clucocorticoid should be avoided!
Reactive arhtritis 1 • Inflammatory arthritis, which occasionally follows certain GI or genitourinary infections • Reiter sdr = arthritis + conjuctivitis + urethritis • Most common after • Chlamydia trachomatis, Shigella flexneri, Salmonella species, Yersinia enterocolitica, Campylobacter jejuni • Genetic predisposition • HLA-27 positive 60-80%
Reactive arthritis 2 • Clinical Presentation • Asymmetric oligoarthritis • Urethritis • Conjuctivitis • Skin and mucous lesions • Usually transient, lastin one to several months • Some patients develope chronic arthritis
Reactive arthritis 3 TREATMENT • Control of pain and inflammation! • NSAIDs • Severe cases short glucocorticoid therapy • Ophthalmologic referral if you suspect iritis • Remember and search for infection! • Clamydia tr • Antibiotic treatment if still needed • Prolonged antiobiotic therapy has NOT been showed to be beneficial
Crystal-Induced Arthritis 1 • Gout (Urate crystals) • Pseudogout (Calcium pyrophosphate dihydrate crystals) • Apatite disease • Gout arthritis developes when urate crystals deposites in the joints • Primary: hyperuricemia due to undersecretion of uric acid • Secondary: Renal disease, diuretic therapy, low-dose aspirin, ethanol, starvation, lactic asidosis, dehydration, pre-eclampsia, diabetic ketoasidosis
Crystal Induced Arthritis 2 • Clinical Presentation • Excruciating pain • Usually in single joint in foot or ankle • Occasionally a polyarthritic oncet can mimic rheumatoid arthritis • Joint is swollen, skin erythema, warm/hot • Chronic gout: With time acute gouty attacs more often, even chronic joint deformity may appear • Lab: Uric acid levels with 70%, Crystals seen in the joint fluid examined with microscope
Crystal Induced Arthritis 3 TREATMENT • Acute gout • NSAID high dose • Indomethacin 75 mg start then 50 mg every 6 hours 24 hrs, 50 mg TDS 24 h, 25 mg TDS 24 h • Diclofenac 75 mg BDS • Ibuprofen 400-800 mg TDS • Glucocorticoids (especcially when NSAID is contraindicated) • Intra-articular injection • Prednison 40 mg OD 3-5 days • Colchisine • 1 mg stat followed 0,5 mg every 2 hours orally until patient improves or ad 10 mg • Prevention • Anti-hyperuricaemic therapy; Allopurinol • Goal serum uric acid below 8 mg/dl (0.48 mmol/l) • Avoid precipitants (alcohol, small fish, diuretics) • Reduce weight in obese patients Remember that allopurinol can make acute gout even worse! Start after clinical improvement!
Infectious Arthritis 1 • Septic infection! • Non-conococcal: Staphylococcus Aureus, Streptococci • Conococcal arthritis • Occasionally: M Tuberculosis, Brucella, Fungi • Non-bacterial infectious arthritis • Viral infections: Hepatitis B, Rubella, Mumps, Mononucleosis, parvovirus, enterovirus, adenovirus
Infectious Arthritis 2 • Clinical Presentation • Non-gonococcal infectious arthritis • Fever • Acute monoarticular arthritis • Multiple joint may be affected by hematogenous spread of pathogens • Gonococcal arthritis • Migratory or additive polyarthralgias followed by tenosynovitis or arthritis of wrist, ankle or knee and vesicopustular skin lesions
Infectious Arthritis 3 TREATMENT • Immediate antibiotic therapy • Cover S. Aureus, Streptococcus, Neisseria gonorrhoeae • IV-antibiotics are recommended for at least 2 weeks, followed by oral antibiotics 2(-4) weeks • When definite gonococcal arthritis Ceftriaxone i.v. For 3 days followin 7-14 days treatment with cefixime or Amoxicillin/clavulanate • Surgical drainage especcially if there is big joint (shoulder, hip), lobulation of pus, osteomyelitis or delay with response to treatment • Supportive treatment for septic infection! • NSAID
HIV-infection and arthritis 1 • HIV-associated arthralgia • Any stage of HIV infection • Mild to moderate, involves usually large joints (shoulders, elbows, knees) • No synovitis! • Treatment: Pain medication, support
HIV-infection and arthritis 2 • Reactive arthritis • Psoriatic arthritis • HIV-assosiated arthritis • Virus is directly involving joint synovium • Oligoarticular, occurs predominantly in the lower extremities • Self-limiting course, lasting <6 weeks • X-ray: no erosion in the joints • Also HIV-associated polyarthritis is possible, resembles rhematoid arthritis • Synovitis abates when CD4 is declining, but joint destruction continues
Diagnose with intra-articular puncture Main principles • Clear synovial fluid: Osteoarthritis, Rheumatoid arthritis • Leukocyte amount • Thick, fuzzy: Crystal-induced Arthritis • Crystals seen in microscope • Purulent: Infectious arthritis • Culture, Gram stain Assure that your technique is clean!
Take Home Message • Osteoarthritis is the most common reason for joint pain; treat the pain and educate the patient • Treat with antibiotics when… • It’s infectious arthritis! • Reactive arthritis if there still is infection • If you suspect Rheumatoid arthritis, treat aggressively, consider refferal for specialist Asante, Thank you!