Download
1 / 34
370 likes | 670 Vues
Implementing Computer-Assisted Coding. A study of the pioneers (results and tips from 5 implementations). Sponsored by:. The problem to be solved. ICD-10 will challenge coders productivity . Initially, 50-70% according to AHIMA studies & experience in Canada

E N D
Implementing Computer-Assisted Coding A study of the pioneers (results and tips from 5 implementations) PHIMA Annual Meeting
Sponsored by: PHIMA Annual Meeting
The problem to be solved • ICD-10 will challenge coders productivity. Initially, 50-70% according to AHIMA studies & experience in Canada • Yet there is already a coder shortage • Failure to address this problem will lead to a negative Revenue Cycle impact HIMSS. ICD-10 Lessons Learned from Canada 12/09 ICD-10 Task Force
Two possible solutions • Hire more coders • Where do we find them? • How do we pay for them? • Leverage technology • Will it work for us? • CAC has the potential to increase coder productivity by 25 – 60% • AHIMA e-HIMTM Work Group on Computer-Assisted Coding
Demystifying Computer Assisted Coding • What is CAC? • Does it live up to the claims? • Is it right for my organization? • What ensures success? • Should I become an advocate?
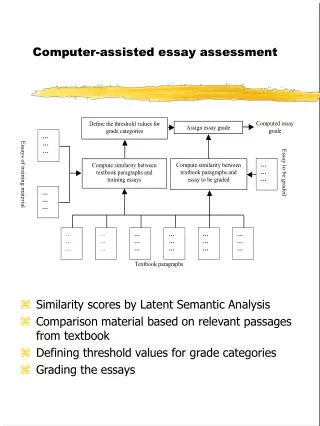
What is CAC? The CAC Natural Language Processor (NLP) reviews the patient record and identifies medical language found within the text of the documented patient encounter. • Software can ‘read’ physician documentation • Free form text is processed • Does not require structure or changes in physician behavior • Physicians use standard dictation/transcription, speech recognition, or templates with free-text fields • Exception: cannot process handwritten free-text • NLP converts patterns of language into correct codes
How does it “read” documentation? For example: • Patient presents with a pressure ulcer due to diabetes. • Patient had a MI in 2005. • Patient’s mother has hypertension. • Patient appears to have a depressed fracture.
How does it “read” documentation? The CAC engine finds terms: • Patient presents with a pressure ulcer due to diabetes. • Patient had a MI in 2005. • Patient’s mother has hypertension. • Patient appears to have a depressed fracture.
How does it “read” documentation? Finds terms and puts them in context: • Patient presents with a pressure ulcer due to diabetes. • Patient had a MI in 2005. • Patient’s mother has hypertension. • Patient appears to have a depressed fracture.
CAC becomes Coder Command Central Human Coder is presented with electronic charts with suggested codes. Core Clinical Documentation for coding compliance ENCODERexisting coder tools integrated Billing & Abstraction Systemall codes and info sent from CAC ADTwhen the patient is registered ADT info is sent to CAC Results Archive Annotated documents stored for future reference
Butler’s Motivation for CAC • Mitigate increasing workload • Added 13 IRG facilities (lab & radiology) • Increased from 7000 to 8700 records/week • ICD-10 training tool • Dual coding of both ICD-9 and ICD-10 one year prior October 2014 • Continued documentation gap analysis • Dual coding data collection • Coding audit trails for RAC • QA workflow
Butler’s Benefits Realized • 83% of lab work gets automated, 50% overall • Reassigned 1.6 FTEs • Coders able to address more complicated charts and move on to inpatient training • Decrease of 2 AR Days • Dropped bill hold from 4 to 2 days On Mondays 4,800 bills get dropped instead of 1,000 since coding automation can now occur on weekends.
RWJ’s Motivation for CAC “The Paper Chase” • Outpatient reports routed to HIM via interoffice mail • Ancillary departments with stand alone systems • Manual coding from financial system reports
RWJ’s Success Story • Eliminated “The Paper Chase” • Outpatient turnaround time improved by 80% • Reduced coding consultant expenses • Coder education & training • Coder efficiency • Coder recruitment • Improved DNFB • Improved coding workflow • Distribution of coding work. • Coding skill level, new coders
Ohio Health’s Motivations for CAC • Maximize coder efficiency – Streamline workflow – Reduce time to complete case • Improve coding quality – Increase accuracy (lessen denials and rework) – Gain consistency within the coding department • Improve case mix index • Shorten revenue cycle Source: AHIMA presentation September 30, 2012 by Diane Setty, RHIA, CPHQ, System Director, HIM OhioHealth
Ohio Health’s Results • Significant productivity gains • Enhanced ability to monitor productivity • Enhanced clean claim rate • Streamlined coder work • through integrating applications [EMR, encoder, and billing system] into one view • Enhanced capability to audit code assignment Source: AHIMA presentation September 30, 2012 by Diane Setty, RHIA, CPHQ, System Director, HIM OhioHealth
Adventist Health System • Deployed Since 2010 • 40+ Hospitals • 250+ Coders • 58% Productivity Increase • Claims Denials Reduced by 80% • Process Reduced by 2 Days • Dual Coding ICD-9 and ICD-10 Coding, LIVE since 10/2012
Other Hospital Initiatives Financial Improvements Benefits realized by CAC Pioneers • Better coder productivity • Inpatient 20-40% • Outpatient 80% • Reduce AR days • Reduce AR days by 2 days • Reduce denials • Claims Denials reduced by as much as 80% • Medical necessity edits • Improve case mix • Staff management tool • Work assignment tool • Coder education and training (especially ICD-10) • Staff recruitment tool • Coding accuracy • Quality 98-100% Accurate • Reduce paper • CDI initiatives
Other Potential Benefits of CAC • Reduce expenses • Outsourced coders • Coder overtime • Coder recruitment/retention • Improve compliance • Ease the transition to ICD-10 • Generate problem list • Improve documentation quality
Tip#1 Coders will continue to be a precious commodity • Certain aspects of CAC rely on coder verification, validation, and approval. • Coders roles may change. They will be elevated to the role of an editor. • Coders can be freed up from mundane tasks and placed in the most challenging areas of Health Information Management. • Encourage coder participation into the integration of CAC tool
Tip#2 Get going and get the most from CAC • Get started early • More time = more options available to you • Enlist expertise • No time for trial and error • Use a solid plan based on proven methodology • Most expedient path • Fewer “surprises”
Tip#2a Work to be done by Oct 1, 2014 • Budget cycle • Vendor selection • Contracting • Planning • Implementation team • Software install • Interfacing documents • Testing • Training • Tuning
Tip#3 CAC can be affordable (but do your homework) • Check references • Check demo for fit with your workflow • Go on a site visit • Utilize an Return-On-Investment (ROI) worksheet
Tip#4 Document the goalsto guide you • Use them to drive your activities • Use them to align your team • Use them to make your decisions In absence of clearly defined goals, we become strangely loyal to performing daily acts of trivia.Author Unknown
Tip#5 “ITis a team sport” (my former boss) CAC: • is Information Technology • may be a tool for coders but to be successful you need support from others
Tip#5a Establish a steering committee • Include: • An Executive Sponsor • C-Suite Support • IT (need a partnership) must continually build that relationship • Coding manager • Consider: • Physician Liaison • Quality • Business Office Rep • Get acceptance for: • Goals • Budget • Meetings & Reports • Project Governance • Their commitment and time You’ll want their support when the going gets rough …and it will get rough
Tip#5b Team members for inclusion Committed • Project Manager (PMO) • Coding Management • Coders • Data Quality • IS • Database team • Interface Team • Desktop Team • Virtual Access Team • Information Security • Server Team Involved • Medical Staff • Compliance • Legal • Business Office Staff • Registration • CAC Vendor • Other members of HIM team • ICD-10 team • EHR team
Tip#6 Motivate and succeed • Set clear expectations • Ensure communication is open, honest, and respectful • Foster a strong sense of belonging to the group • Take advantage of differences • Make sure members are comfortable enough to take reasonable risks (i.e. trust) • Have process for resolving conflicts Ask not what your teammates can do for you. Ask what you can do for your teammates. Magic Johnson
Tip#7 HIM has a key leadership role “Computer Assisted Coding (CAC) with Natural Language Processing (NLP) will soon be integrated into the coding workflow of every organization.” “The challenge for health information management (HIM) is to leverage the technology by demonstrating its value and championing its use for additional purposes. AHIMA, Embracing CSC Beyond Reimbursement Initiatives, November 2012
Embrace the role of catalyst Marilyn Marchant’s email: mmmarchant@msn.com


![Computer Assisted Learning [CAL]](https://cdn2.slideserve.com/3962806/slide1-dt.jpg)