Download
1 / 18
200 likes | 840 Vues
Headache and Facial Pain Tintinalli Chapter 227. Headache. 4% of all ED visits 3.8% of all headaches are from serious pathology primary cause of 150 million lost workdays and 329,000 lost school days each year in the United States Usually divided into primary and secondary Headache syndromes

E N D
Headache • 4% of all ED visits • 3.8% of all headaches are from serious pathology • primary cause of 150 million lost workdays and 329,000 lost school days each year in the United States • Usually divided into primary and secondary Headache syndromes • Primary: cluster, migraine, tension
ACEP Headache Categories • Secondary Headaches • Critical secondary causes requiring emergent identification and treatment • Critical secondary causes not necessarily requiring emergent identification or treatment • Generally benign and reversible secondary causes
Critical Secondary Subarachnoid Intraparenchymal Epidural Subdural Stroke Carvernous Sinus Thrombosis Stroke AV malformation Temporal Arteritis Artery dissection Meningitis Encephalitis Abscess Tumor Pseudotumor cerebri Ophthalmic Glaucoma Iritis Opitic Neuritis Nitrates & nitrites MOA inhibitors ETOH withdrawal Carbon monoxide poisoning Pheochromocytoma Hypoxia Hypoglycemia Hypercapnia High Altitude cerbral edema Preeclampsia Non Critical Secondary Sinusitis Odontogenic Otic Chronic analgesic use Post Lumbar puncture Headache - secondary
Where To Start • History • Patients with an atypical history • a substantial change from a previous headache pattern • or certain high-risk features require emergency department evaluation
History - continued • Pattern: first severe headache, worst headache ever, steady worsening over several days, or significant differences from prior headaches in terms of duration, severity, or associated symptoms • Onset: Sudden-onset headache, especially if it begins during exertion (including coughing, defecation, etc.) • Location: nonspecific and should not be relied on for diagnosis • Associated Symptoms: history of syncope, altered level of consciousness, confusion, neck pain or stiffness, persistent visual disturbance, fever, or seizure; search for symptoms of nonneurologic conditions causing headaches • Medications: nitroglycerin, chronic analgesic use, monoamine oxidase inhibitors (MAOIs), or anticoagulants • Family History: relatives with SAH because the risk of ruptured intracranial aneurysm in first- and second-degree relatives is up to four times higher than in the general population
Special Groups • Women – higher % migraines (Menarche, menstruation, oral contraceptive use, pregnancy, and menopause all may affect migraine) • Pregnancy - Preeclampsia should be considered in pregnant women. Pregnancy improves migraine symptoms in 60 to 70 percent of patients • Elder - New onset of headaches in patients over 50 years of age is worrisome and may herald the presence of a secondary cause
Physical Examination • Vital Signs • Fever – meningitis, sinusitis, SAH, encephalitis, HIV/AIDS • Sinus tenderness; Temporal Arteries, Eyes/Fundoscopy, Ears, Mastoids, Dentition, Neck Muscles, & Complete Neurologic Examination
Diagnostics • CT • Neuroimaging should be considered in patients with nonacute headache and an unexplained abnormal finding on neurologic examination • headache worsened by Valsalva, causing awakening from sleep, new headache in older population, or progressively worsening headache • atypical migraine features or in patients who do not fulfill the strict definition of migraine • LP • Suspected SAH, Meningitis, Encephalitis • contraindications to LP include the suspicion of raised ICP, which can be excluded by a combination of the absence of papilledema, normal level of consciousness, and normal findings on neurologic examination • MRI • cost and restricted availability of MRI limit its utility in the emergency investigation • No more sensitive then CT for SAH • More sensitive for diffuse axonal injuries, small parenchymal contusions, isodense subdural hemorrhages, and most tumors
Primary Headaches • Migraine • 5% of males & 15% of females • Migraine w/o aura accounts for most • Onset is slow and duration is 5-72 hours • Nausea, Vomiting, & Photophobia are common • Aura – usually < 60 min; vision symptoms most common • TX: pick your potion • DHE (1mg IV over 3min); Imitrex (6mg SC); Toradol (30mg IV or 60mg IM); Droperidol (2.5mg IV); Reglan (10mg IM/IV); Compazine (10mg IV/IM); Benadryl (25-50mg IV/IM); Fluids
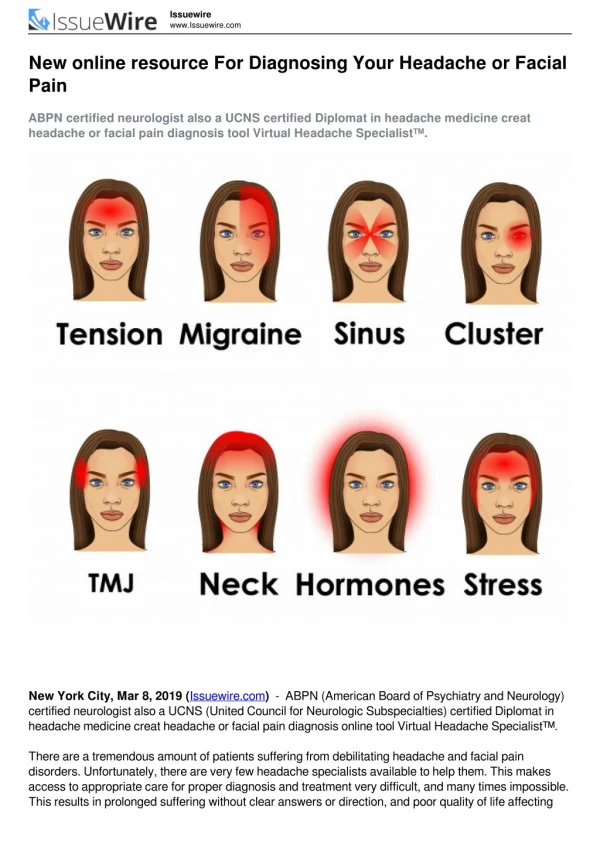
Primary Headaches • Tension Type • Bilateral, nonpulsating, not worsened by exertion, and not associated with nausea or vomiting • TX: NSIADS, OMT! • Cluster • 0.4% of the population; usually in men and onset >20 yo • Severe unilateral orbital/supraorbital/temporal pain lasting 5-180 minutes • Pain associated with at least one of the following: injection, lacrimation, nasal congestion, rhinorrhea, facial swelling, miosis, or ptosis • Occur in clusters over a day to week • TX: high flow O2 effective in up to 70%; DHE & Imitrex also approved for use
Life Threatening Headaches • SAH • Incidence 1 per 10,000 • Up to 50% have a normal neurologic examination including neck stiffness • Occur in young population with a median age of 50, & 50% 6 month mortality rate • Occipitalnuchal pain is most common • CT has 93% sensitivity if presentation in 1st 24 hours • Offering LP with negative CT is mandatory • Xanthochromia on LP is the Gold Standard & very sensitive if onset > 12 hours • Traumatic Taps present in 20%, persistent blood warrants CNS vascular imaging • TX: reverse anticoagulation; BP usually lowered to 140mmHg if normal LOC; nimodipine (60mg PO/NG q 4 h); seizure proph. per consultant
Life Threatening Headaches • CVA • Headache and neurologic findings • 55% of bleeds present with headache • 17% of ischemic CVAs have headache • Brain Tumor • 70% of patients complain of headache • Can be worse at night, positional, nausea & vomiting • Meningitis • Headache, fever, neck stiffness • LP with the above presentation • Don’t withhold antibiotics • Antivirals should be initiated if suspected
Secondary Causes • Temporal Arteritis • Over 50; more common in women; incidence is 3 per 10,000 • Severe & throbbing frontotemporal headache; jaw claudication; associated with Polymalgia Rheumatica • Dx(3 of 5): over 50, new-onset localized headache, ESR >50, tender Temporal artery or decreased pulse, abnormal artery biopsy • Prednisone 40-60mg per day and urgent follow-up
Secondary Causes • HTN • Treat if no secondary headache syndromes suspected • POST LP Headache • 10-36%, 1-48 hours after procedure • NSAIDS, fluids, caffeine, blood patch • Dissection • Usually present with neurologic signs/sym • Median age is 40 yo • Diagnosis via angiography/CTA/MRA • Pseudotumor Cerebri • Wacky/Wobbly/Wet • Young/Obese/Headaches may be chronic • Usually normal LOC, papilledma, normal CT, increased opening pressure on LP • TX: acetazolamide & referral
Facial Pain • Temporomandibular Disorder • Persistent discomfort due to dysfunction of the TMJ, surrounding muscles, and ligaments • TMJ noise and pain on movement, limited jaw movements, locking of the jaw on opening, bruxism, Headaches • DX: x rays have little value; non-emergent MRI is the pest imaging test • Treatment: NSAIDS for initial treatment and referral
Facial Pain • Trigeminal Neuralgia (Tic Douloureux) • Paroxysms of severe unilateral pain in the trigeminal nerve distribution lasting only seconds, with normal findings on neurologic examination • Paroxysms are usually short • Carbamazepine (Tegretol) should be initiated @ 200 mg divided BID; usually dose 400-800mg divided BID • Neurologic Referral
Resources • Tintinalli Chapter 227 • UptoDate