Download
1 / 22
220 likes | 361 Vues
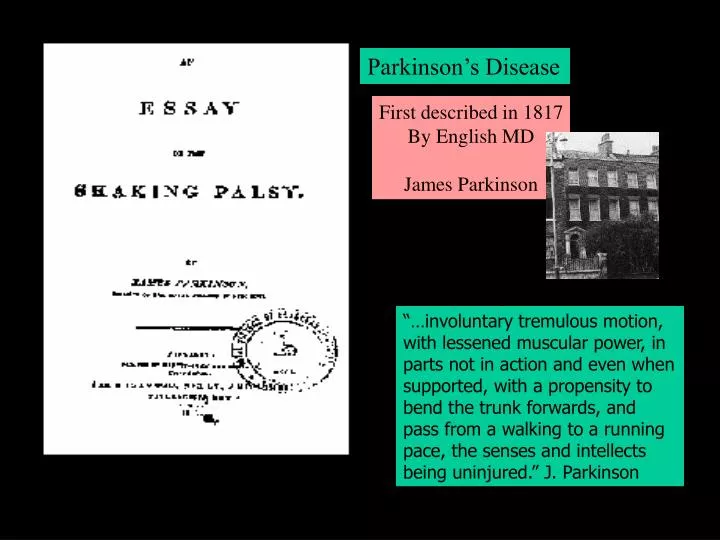
Parkinson’s Disease. First described in 1817 By English MD James Parkinson. 1817 by James Parkinson.

E N D
Parkinson’s Disease First described in 1817 By English MD James Parkinson • 1817 by James Parkinson “…involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported, with a propensity to bend the trunk forwards, and pass from a walking to a running pace, the senses and intellects being uninjured.” J. Parkinson
PD: Motor System Disorder • Chronic • Progressive • Non Fatal • 1 to 1.5 million cases in the US • strikes 1 in every 100 over 50 • Equal opportunity disease… • men, women all ethnicities • slightly higher rate among • whites vs blacks Disease of Aging – onset 55 (idiopathic) Early Onset: 5-10% diagnosed
Idiopathic 400,000 nigral cells in SN 2,400 cells die each year (Apoptosis)…100 X 2,400 = 240,000 …50% cell death = mild symptomolgy • So PD accelerated…why? • environmental? • genetic? • Head injury (parkinsonism)
Monozygotic Dizygotic
Parkinson's Disease •Lewy body in a substantia nigra neuron Caused by alpha synuclein & Parkin: gene responsible for making these proteins suspect early onset
Environmental… Pesticides Herbicides Insectcides Well-Drinking Water Rural Living Higher incidence in agriculture workers…. Environmental… Metals: Manganese Copper Aluminum
Basal Ganglia Striatum Nigrostriatal Pathway Dopaminergic Cell bodies 80% die – degeneration of pathway..bingo NO Dopaminergic transmission
Parkinson’s Disease Globus Pallidus Substantia Nigra Caudate & Putamen Sub Thalamic Nuclei Disease of the Basal Ganglia Facilitates Movement D1 Inhibits Movement D2
D2 receptors neurons from putamen fire excessively…loss of control of motor function Excitatory: green -- Inhibitory: red 1. Substantia Nigra axons inhibit the putamen 2. Axon loss increases excitation in Globus Pallidus 3. Globus Pallidus has increased inhibition to Thalamus 4. Then decreased excitation from the Thalamus to Cortex
Symptoms 1. Rigidity • Muscular stiffness and increased muscle tone • Patients usually unaware of rigidity, but troubled with slowness • More apparent to doctor than patient • Cogwheeling – ratchet like movement 2. Hypokinesia & 3. Bradykinesia • Hypokinesia: inability to initiate a voluntary movement • Bradykinesia: slowness of movement • Decrease in: • Eyeblink • Facial expression • Eating and chewing
4.Tremor • An involuntary movement: head, limbs, or entire body • Most apparent when limb is rested and supported • Increases with stress • Ceases during sleep • Decreases with intentional movements • 'Pill rolling tremor' if most prominent in fingers & hand • Most bothersome, yet least disabling of all symptoms
Stage 1 • Symptoms mild - inconvenient • Unilateral • Tremor- leans to affected side • Affected arm in semiflexed position with tremor • Stage 4 • Significant disability • Institutionalization • Stage 2 • Symptoms mod – disability min • Bilateral • Early postural changes • Slow, shuffling gait • Toe-gait walk • Stage 3 • Symptoms mod severe • Major posture problems - • stooped, knees flexed while walking • Major balance problems - • unsteadiness while turning • Falls • Severe tremor, rigidity or bradykinesia • Stage 5 • Loss of global ability • Bradykinesia very severe • Cannot walk or stand
Treatment….. HEY LETS JUST GIVE DOPAMINE!!!
Dopamine doesn’t cross the blood brain barrier…. But levodopa does (l-dopa)! Problems: 1. doesn’t address the cell death 2. in time l-dopa is not effective (good for early to intermediate stages) Phenylalanine Tyrosine L- Dopa Dopamine Aromatic L amino acid decarboxylase • Sinemet (l-dopa+carbidopa) • l-dopa quickly converted to DA • in PNS decarboxylase inhibtor • 75% respond to drug
Selegiline (MAOI) • Delays Parkinsonian disability and the need for levodopa therapy by 9-12 months • Inhibits dopamine degradation • allows for 20% smaller doses of levodopa • Exacerbation of levodopa-associated side effects • Insomnia, postural hypotension • inhibiting monoamine oxidase-B morepre-synaptic dopamine • Also…inhibits this enzyme …converts MPTP to MPP+ (bad stuff)
“on-off” of PD “I need to explain the "on-off" phenomenon. This Jekyll and-Hyde melodrama is a constant vexation for the P.D. patient, especially one as determined as I was to remain closeted. "On" refers to the time when the medication is telling my brain everything it wants to hear. I'm relatively loose and fluid, my mind clear and movements under control. Only a trained observer could detect my Parkinson's. During one of my "off" periods, even the most myopic layperson, while perhaps not able to diagnose P.D. specifically, can recognize that I am in serious trouble.” -Michael J. Fox, an excerpt from Lucky Man http://www.michaeljfox.org/
Thalamotomy: remove thalamus (M.J. Fox - 1998) Pallidotomy: remove the globus pallidus • Helps the symptoms of tremor, dyskinesia, rigidity & bradykinesia • however, irreversible destruction of brain tissue • Overtime the benefits decline • May compromise other intact brain processes: speech, vision etc. New Treatment Strategy…..DBS (deep brain stimulation) - US Food and Drug Administration recently approved (Jan. 15, 2002) - Tiny electrodes on the scalp – connecting wire to implanted pulse generator under the collarbone - 80% reduction of tremor & bradyk. - can modify stimulation based on severity of symptoms
DBS • Thalamus • Globus pallidus • Sub Thalamic • (best) • Thalamus: tremor, safer then • lesion • Globus pallidus: dyskinesia • safer than lesion • Sub Thalamic: improve all • Symptoms • improvement of motor scores • 40-60% during “off” • 10% during “on”
Parkinson’s Disease (long-term) Striatum Substania Nigra Lesioning – Neurotoxicity
Parkinson’s Disease – (acute: manipulation of pharmacological agent) Fluphenazine – D2 Dopaminergic Antagonist Blockade of receptor TARGET STRIATUM (D2) HYPOKINESIA