Download
1 / 1
10 likes | 144 Vues
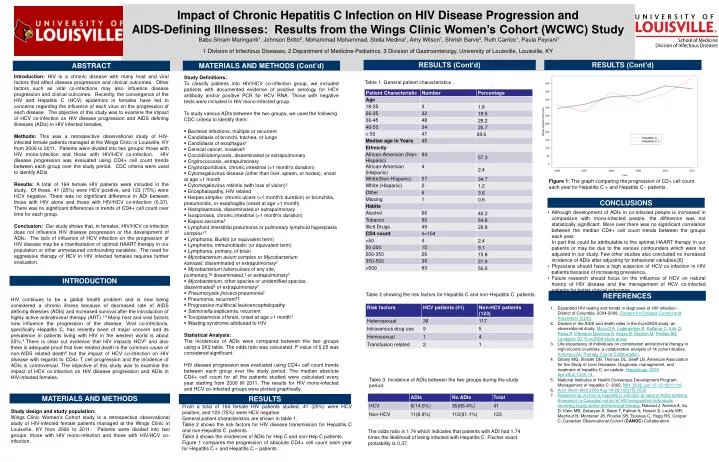
Impact of Chronic Hepatitis C Infection on HIV Disease Progression and AIDS-Defining Illnesses: Results from the Wings Clinic Women’s Cohort (WCWC) Study

E N D
Impact of Chronic Hepatitis C Infection on HIV Disease Progression and AIDS-Defining Illnesses: Results from the Wings Clinic Women’s Cohort (WCWC) Study BabuSriram Maringanti1, Johnson Britto2, Mohammad Mohammad, Stella Medina1, Amy Wilson1, Shirish Barve3, Ruth Carrico1, Paula Peyrani1 1 Division of Infectious Diseases, 2 Department of Medicine-Pediatrics, 3 Division of Gastroenterolgy, University of Louisville, Louisville, KY RESULTS (Cont’d) RESULTS (Cont’d) MATERIALS AND METHODS (Cont’d) ABSTRACT Introduction: HIV is a chronic disease with many host and viral factors that affect disease progression and clinical outcomes. Other factors such as viral co-infections may also influence disease progression and clinical outcomes. Recently, the convergence of the HIV and Hepatitis C (HCV) epidemics in females have led to concerns regarding the influence of each virus on the progression of each disease. The objective of this study was to examine the impact of HCV co-infection on HIV disease progression and AIDS defining illnesses (ADIs) in HIV infected females. Methods: This was a retrospective observational study of HIV-infected female patients managed at the Wings Clinic in Louisville, KY from 2006 to 2011. Patients were divided into two groups: those with HIV mono-infection and those with HIV/HCV co-infection. HIV disease progression was evaluated using CD4+ cell count trends between each group over the study period. CDC criteria were used to identify ADIs. Results: A total of 164 female HIV patients were included in the study. Of these, 41 (25%) were HCV positive, and 123 (75%) were HCV negative. There was no significant difference in ADI between those with HIV alone and those with HIV/HCV co-infection (0.37). There was no significant differences in trends of CD4+ cell count over time for each group. Conclusion: Our study shows that, in females, HIV/HCV co-infection does not influence HIV disease progression or the development of ADIs. The lack of influence of HCV infection on the progression of HIV disease may be a manifestation of optimal HAART therapy in our population or other unmeasured confounding variables. The need for aggressive therapy of HCV in HIV infected females requires further evaluation. • Study Definitions: • To classify patients into HIV/HCV co-infection group, we included patients with documented evidence of positive serology for HCV antibody and/or positive PCR for HCV RNA. Those with negative tests were included in HIV mono-infected group. • To study various ADIs between the two groups, we used the following CDC criteria to identify them: • Bacterial infections, multiple or recurrent • Candidiasis of bronchi, trachea, or lungs • Candidiasis of esophagus† • Cervical cancer, invasive§ • Coccidioidomycosis, disseminated or extrapulmonary • Cryptococcosis, extrapulmonary • Cryptosporidiosis, chronic intestinal (>1 month's duration) • Cytomegalovirus disease (other than liver, spleen, or nodes), onset at age >1 month • Cytomegalovirus retinitis (with loss of vision)† • Encephalopathy, HIV related • Herpes simplex: chronic ulcers (>1 month's duration) or bronchitis, pneumonitis, or esophagitis (onset at age >1 month) • Histoplasmosis, disseminated or extrapulmonary • Isosporiasis, chronic intestinal (>1 month's duration) • Kaposi sarcoma† • Lymphoid interstitial pneumonia or pulmonary lymphoid hyperplasia complex*† • Lymphoma, Burkitt (or equivalent term) • Lymphoma, immunoblastic (or equivalent term) • Lymphoma, primary, of brain • Mycobacterium avium complex or Mycobacterium kansasii, disseminated or extrapulmonary† • Mycobacterium tuberculosis of any site, pulmonary,†§ disseminated,† or extrapulmonary† • Mycobacterium, other species or unidentified species, disseminated† or extrapulmonary† • Pneumocystisjirovecii pneumonia† • Pneumonia, recurrent†§ • Progressive multifocal leukoencephalopathy • Salmonella septicemia, recurrent • Toxoplasmosis of brain, onset at age >1 month† • Wasting syndrome attributed to HIV • Statistical Analysis: • The incidences of ADIs were compared between the two groups using a 2X2 table. The odds ratio was calculated. P value of 0.05 was considered significant. • HIV disease progression was evaluated using CD4+ cell count trends between each group over the study period. The median absolute CD4+ cell count for all the patients studied were calculated every year starting from 2006 till 2011. The results for HIV mono-infected and HCV co-infected groups were plotted graphically. Table 1. General patient characteristics . • . Figure 1: The graph comparing the progression of CD+ cell count each year for Hepatitis C + and Hepatitis C - patients. CONCLUSIONS • Although development of ADIs in co-infected people is increased in comparison with mono-infected people, the difference was not statistically significant. More over there was no significant correlation between the median CD4+ cell count trends between the groups each year. • In part this could be attributable to the optimal HAART therapy in our patients or may be due to the various confounders which were not adjusted in our study. Few other studies also concluded no increased incidence of ADIs after adjusting for behavioral variables.[6] • Physicians should have a high suspicion of HCV co-infection in HIV patients because of increasing prevalence. • Future research should focus on the influence of HCV on natural history of HIV disease and the management of HCV co-infected patients for better clinical outcomes. INTRODUCTION • HIV continues to be a global health problem and is now being considered a chronic illness because of decreased rate of AIDS defining illnesses (ADIs) and increased survival after the introduction of highly active antiretroviral therapy (ART).1-3 Many host and viral factors now influence the progression of the disease. Viral co-infections, specifically Hepatitis C, has recently been of major concern and its prevalence in patients living with HIV in the western world is about 25%.4 There is clear cut evidence that HIV impacts HCV5 and also there is adequate proof that liver related death is the common cause of non-AIDS related death6 but the impact of HCV co-infection on HIV disease with regards to CD4+ T cell progression and the incidence of ADIs is controversial. The objective of this study was to examine the impact of HCV co-infection on HIV disease progression and ADIs in HIV-infected females. Table 2 showing the risk factors for Hepatitis C and non-Hepatitis C patients. REFERENCES Expanded HIV testing and trends in diagnoses of HIV infection - District of Columbia, 2004-2008. Centers for Disease Control and Prevention (CDC). Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Mocroft A, Ledergerber B, Katlama C, Kirk O, Reiss P, d'ArminioMonforte A, Knysz B, Dietrich M, Phillips AN, Lundgren JD; EuroSIDA study group Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Antiretroviral Therapy Cohort Collaboration. Ghany MG, Strader DB, Thomas DL, Seeff LB, American Association for the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009 Apr;49(4):1335-74. National Institutes of Health Consensus Development Program. Management of hepatitis C: 2002. NIH. 2002 Jun 10-12:19(1):116 Arch Intern Med 2006 Aug 14-28;166(15):1632 Relationship of chronic hepatitis C infection to rates of AIDS-defining illnesses in a Canadian cohort of HIV seropositive individuals receiving highly active antiretroviral therapy.Raboud J, Anema A, Su D, Klein MB, Zakaryan A, Swan T, Palmer A, Hosein S, Loutfy MR, Machouf N, Montaner JS, Rourke SB, Tsoukas C, Hogg RS, Cooper C; Canadian Observational Cohort (CANOC) Collaboration. Table 3. Incidence of ADIs between the two groups during the study period. MATERIALS AND METHODS RESULTS . • From a total of 164 female HIV patients studied, 41 (25%) were HCV positive, and 123 (75%) were HCV negative. • General patient characteristics are shown in table 1. • Table 2 shows the risk factors for HIV disease transmission for Hepatitis C and non-Hepatitis C patients. • Table 3 shows the incidences of ADIs for Hep C and non-Hep C patients. • Figure 1 compares the progression of absolute CD4+ cell count each year for Hepatitis C + and Hepatitis C – patients . Study design and study population: Wings Clinic Women’s Cohort study is a retrospective observational study of HIV-infected female patients managed at the Wings Clinic in Louisville, KY from 2006 to 2011. Patients were divided into two groups: those with HIV mono-infection and those with HIV/HCV co-infection. The odds ratio is 1.74 which indicates that patients with ADI had 1.74 times the likelihood of being infected with Hepatitis C. Fischer exact probability is 0.37.