Download
1 / 43
430 likes | 558 Vues
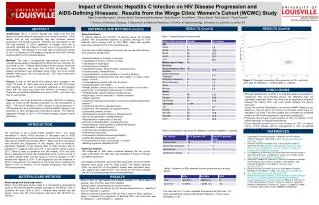
Impact of Contraception on HIV Acquisition, Disease Progression, and Viral Shedding. Elizabeth Stringer MD, MSc Center for Infectious Disease Research in Zambia, Lusaka, Zambia University of Alabama at Birmingham. The face of the HIV epidemic. Maternal Mortality sub-Saharan Africa.

E N D
Impact of Contraception on HIV Acquisition, Disease Progression, and Viral Shedding Elizabeth Stringer MD, MSc Center for Infectious Disease Research in Zambia, Lusaka, Zambia University of Alabama at Birmingham
Maternal Mortality sub-Saharan Africa Shah et al Reproductive Health Matters 2007
Does hormonal contraception affect: HIV disease acquisition? HIV disease progression? HIV shedding?
Does hormonal contraception affect: HIV disease acquisition? HIV disease progression? HIV shedding?
HIV acquisition HC-HIV Study • Prospective study • 6,109 HIV-negative women • Thailand, Uganda, Zimbabwe • Women were on method at entry • 3 monthly follow-up for 15-24 months • Outcome: HIV acquisition • 213 seroconversions (2.8 / 100 woman years) Morrison et al AIDS 2007
HIV acquisition HC-HIV Study: Results *Adjusting for site, living with partner, age, participant behavioral risk, primary partner risk, coital frequency, and condom use. Morrison et alAIDS 2007
HIV acquisition Mombasa Sex Worker Cohort • Open cohort study • HIV-1 negative sex workers • Outcome: incident HIV • Monthly follow-up • 1272 women (> 4,700 woman-yrs follow-up) • 248 seroconversions (8.5 per 100 woman-years) Lavreys et al AIDS 2004
Predictors of HIV acquisition in Mombasa Cohort (n=1272) HIV acquisition Lavreys et al AIDS 2004
HIV acquisition DMPA and HIV Acquisition **About two-thirds DMPA, one-quarter Net-EN users *About two-thirds Net-EN, one-third DMPA users Slide Courtesy of C.Morrison
HIV acquisition OCPs and HIV Acquisition Slide Courtesy of C.Morrison
Does hormonal contraception affect: HIV disease acquisition? HIV disease progression? HIV shedding?
248 seroconversions 161 women had accurate date of seroconversion 91 / 161 HIV seroconversions occurred within one year of a clinic visit when stored samples were HIV-1 RNA and Ab negative 70 / 161 had HIV-1 RNA detected at visit immediately prior to seroconversion Disease Progression Mombasa Cohort and Disease Progression Baeten et al AIDS 2005
Disease Progression Viral load set point • Viral load set point estimated to be established 16 weeks post acquisition • Median set point: 4.46 log10 copies/ml (95% CI 4.32-4.60) • DMPA users had higher set point (+0.33 log 10 copies/ml, p=0.03) Baeten et al JAIDS 2005
Disease Progression Multiple Viral Variants • 89/156 (57%) women had multiple viral variants • More common in women with hormonal contraceptive use (OR 2.7; p=0.003) • Women with multiple viral genotypes • Had higher viral loads 4-24 months after infection (4.84 vs. 4.64 log 10 copies/ml; p=0.04) • Had lower CD4 counts (median 416 vs 617 cells/uL, p=0.01) and a faster decline Baeten et al JAIDS 2005
Disease Progression Viral diversity and disease progression Sagar et al J Virol 2003
Disease Progression Zambia IUD Study • 599 recently-postpartum HIV+ women • Randomized trial • Copper IUD • User-choice hormonal contraception (oral contraceptive pills* or DMPA) • Between June 2002 and Oct 2003 • Outcomes: pregnancy, safety, and switching • Primary outcome: pregnancy * “Mini pill” during early BF; combined preparation thereafter Stringer et al Am J Obstet Gynecol 2007
Disease Progression Enrollment and follow-up • Follow-up every 6 months • CD4+ every 12 mo, but once ART available, every 6 mo • Pregnancy testing and pelvic exam at each visit • PID diagnosed by Hagar’s Criteria • All women followed to pregnancy event, withdrawal, or until last enrolled participant had completed 24 months
Disease Progression Baseline characteristics of cohort
Disease Progression Analysis by Study Arm *Fisher’s exact test
Disease Progression Time to death by randomization arm
Disease Progression Time to CD4 count falling to below 200 cells/uL by randomization arm
Disease Progression Time to either CD4 cell count falling to below 200 cells/uL or death by randomization arm
Time-varying analysis Disease Progression * Cox model with exposure based at start of f/u ** extended Cox model treating contraception as a time-varying covariate. Stringer unpublished data Both models adjusted for initial CD4 count
Disease Progression Other studies HIV disease progression and HC
Does hormonal contraception affect: HIV disease acquisition? HIV disease progression? HIV shedding?
Contraception and HIV infectiousness HIV shedding • Genital HIV-1 shedding used as marker for infectiousness (Pedraza, JAIDS 1999; Baeten, Curr HIV Res 2003) • No association between use of contraception and female-to-male HIV-1 transmission (European Study Group on Heterosexual Transmission of HIV, BMJ 1992) Slide courtesy of Ludo Lavreys
Hormonal contraception and cervical DNA viral shedding HIV shedding
HIV shedding Detection of Cervical HIV-1 DNA Depending on Type of Hormonal Contraception Used OR 12.3 (1.5-101) OR 3.8 (1.4-9.9) OR 2.9 (1.5-5.7) OR 1.0 318 HIV-infected Kenyan women Mostad,Lancet 1997
Risk of SIV Acquisition of Female Monkeys with Progesterone Implants Slide courtesy of C. Morrison Source: Marx (1996); Duerr (1997)
No diff in α-SIV Ab response No IFN-γ secreting cells detectable in Depo-treated arm at 1-2 weeks Response of IFN-γ production delayed in Depo treatment arm Immune responses in macaques treated with SIV and DMPA Trunova Virology 2006
Review • Data on HC and HIV acquisition is varied • HC affected VL set point in new acquisitions • In our RCT women on HC had faster disease progression • Suggestion that DMPA worse than OCPs • Warrants more investigation • HC shown to increase cervical DNA viral shedding
Changes in vaginal environment • Related to vaginal thinning • Vaginal thinning in macaques treated with Progesterone • Marx, Nature 1996 • Slight thinning of vaginal epithelial layer • Miller, AJOG 2000 • Changes in vaginal microenvironment • Progesterone associated with decreased H202+ Lactobacillus • Miller, AJOG 2000
Other possible mechanisms • Increasing HIV co-receptor expression • OCPs upregulates CCR5 receptors in women • Prakash, J of Reproductive Immunology 2002 • Progesterone increases expression of CCR5 and CXCR4 expression • Patterson et al, Int AIDS Conf, 1998 • Infection with multiple viral types • T cell activation
Summary • Ensuring safe and effective contraception to HIV infected women is a priority • Understanding mechanisms of potential interactions between HC and immune system is critical • Evidence to date not compelling to change policy
END • Special thanks to: • Lusaka District Health Board, Lusaka, Zambia • Charles Morrison, FHI • Ludo Lavreys, Tibotech • CIDRZ team • Mike Saag • Sten Vermund • EGPAF
Contraception on immune system function • Estrogen and progesterone decreases immune response (Th1>Th2) • Estrogen increases LTR induced viral replication • Estrogen and progesterone induce upregulation of CCR5 receptor on CD4 T cells in cervical epithelium of non-HIV women- Prakash J of Reproductive Immunology 2002 Enomoto et al JAIDS 2007
Effect of progesterone on chemokine expression in vivo • PBMCs incubated with 50 ng/ml progesterone for 6 days • At 0, 3, and 6 days, RNA was extracted for CCR5, CXCR4, and CCR2b mRNA • Flow cytometry performed to localize increases in CCR5 and CXCR4 Patterson, et al, AJP, 1998