Download
1 / 69
810 likes | 1.49k Vues
New Modes of Mechanical Ventilation. Mazen Kherallah, MD, FCCP Consultant Intensivist King Faisal Specialist Hospital. Key Ideas for Understanding Mechanical Ventilation. Mathematical Models Equation of motion Time constant Mean airway pressure Control Variables Pressure, volume, dual

E N D
New Modes of Mechanical Ventilation Mazen Kherallah, MD, FCCP Consultant Intensivist King Faisal Specialist Hospital
Key Ideas for Understanding Mechanical Ventilation • Mathematical Models • Equation of motion • Time constant • Mean airway pressure • Control Variables • Pressure, volume, dual • Phase Variables • Trigger, Limit and Cycle • Breath Types/Patterns • Optimum Mode Selection
transairway pressure transrespiratory pressure transthoracic pressure volume elastance = Dpressure / Dvolume Lung Mechanics resistance = Dpressure / Dflow flow
Equation of Motion ventilation pressure (to deliver tidal volume) resistive pressure (to make air flow through the airways) elastic pressure (to inflate lungs and chest wall) = + P = Presistive + Pelastance P = R x V + E x V
Phase Variables • Trigger (start)- begins inspiratory flow • Cycling (end)- ends inspiratory flow • Limiting (continue)- places a maximum value on a “control variable” • pressure • volume • flow • time
Trigger Variable- Start of a Breath • Time - control ventilation • Pressure - patient assisted • Flow - patient assisted • Volume - patient assisted • Manual - operator control
Inspiratory - delivery limits • Maximum value that can be reached but will not end the breath- • Volume • Flow • Pressure
End of Insp…cycle mechanisms • The phase variable used to terminate inspiration- • Volume • Pressure • Flow • Time
Breath Type… Only Two (for now)! • Mandatory • Ventilator does the work • Ventilator controls start and stop • Spontaneous • Patient takes on work • Patient controls start and stop
The Control Variable-Inspiratory Breath Delivery • Flow (volume) controlled • pressure may vary • Pressure controlled • flow and volume may vary • Time controlled (HFOV) • pressure, flow, volume may vary
Paw Paw Volume/Flow Control Pressure Control Inspiration Expiration Inspiration Expiration 20 20 Pressure 0 0 2 2 1 0 1 20 20 Volume 0 0 2 2 0 1 0 1 3 3 Flow Time (s) Time (s) 0 0 -3 -3
P aw cmH 0 2 Volume Control Breath Types 60 SEC 1 2 3 4 5 6 -20 120 INSP Flow SEC 1 2 3 4 5 6 L/min 120 EXH If compliance decreases the pressure increases to maintain the same Vt
Dual Control within a Breathvolume-assured pressure support • This mode allows a feedback loop based on the volume • Switches even within a single breath from pressure control to volume control if minimum tidal volume has not been achieved Tbird Bird 8400Sti Bear 1000
Dual Control within a Breathvolume-assured pressure support • The Respiratory Therapist sets : • pressure limit = plateau seen during VC • respiratory rate • peak flow rate (the flow if TV < target) • PEEP • FiO2 • trigger sensitivity • minimum tidal volume
Pressure limit overridden Set pressure limit P aw cmH 0 2 Set tidal volume cycle threshold Tidal volume not met Tidal volume met Inspiratory flow greater than set flow Inspiratory flow equals set flow Flow cycle Set flow limit Switch from Pressure control to Volume/flow control 40 -20 0.6 Volume L 0 60 Flow L/min 60
trigger Pressure at Pressure support no delivered VT ≥ set VT flow= 25% peak yes yes no Insp flow > Set flow Cycle off inspiration yes no Switch to flow control at peak flow setting no delivered VT = set VT PAW <PSV setting yes yes no Control logic for volume-assured pressure-support mode
Dual Control within a Breathvolume-assured pressure support • If pressure too high, all breaths are pressure-limited. • If the peak flow setting is too high , all breaths will be volume-controlled • If the pressure is set too high or the minimum tidal volume is set too low; the volume guarantee is negated • If peak flow set too low, the switch from pressure to volume is late in the breath, inspiratory time is too long.
Dual Control within a Breathvolume-assured pressure support • Amato et al Chest 1992;102: 1225-1234 • Compared VAPS to simple AC volume • Lower WOB • Lower Raw • Less PEEPi
Dual Control Breath-to-Breathpressure-limited flow-cycled ventilationVolume Support • Tidal volume is used as feedback control to adjust the pressure support level • All breaths are patient triggered, pressure limited, and flow-cycled. • Automatic weaning of pressure support as long as tidal volume matches minimum required VT (VT set in a feedback loop to adjust pressure).
Dual Control Breath-to-Breathpressure-limited flow-cycled ventilationVolume Support Maquet Servo-i Servo 300
VS vs VAPS • How does volume support differ from VAPS ? • In volume support, we are trying to adjust pressure so that, within a few breaths, desired VT is reached. • In VAPS, we are aiming for desired VT tacked on to the end of a breath if a pressure-limited breath is going to fail to achieve VT
VS (Volume Support) • Entirely a spontaneous mode • Delivers a patient triggered (pressure or flow), pressure targeted, flow cycled breath • Can also be timed cycled (if TI is extended for some reason) or pressure cycled (if pressure rises too high). • Similar to pressure support except VS also targets set VT. It adjusts pressure (up or down) to achieve the set volume (the maximum pressure change is < 3 cm H2O and ranges from 0 cm H2O to 5 cm H2O below the high pressure alarm setting • Used for patients ready to be “weaned” from the ventilator and for patients who cannot do all the WOB but who are breathing spontaneously
VS (Volume Support) (1), VS test breath (5 cm H2O); (2), pressure is increased slowly until target volume is achieved; (3), maximum available pressure is 5 cm H2O below upper pressure limit; (4), VT higher than set VT delivered results in lower pressure; (5), patient can trigger breath; (6) if apnea alarm is detected, ventilator switches to PRVC
yes Volume from Ventilator= Set tidal volume no calculate compliance Calculate new Pressure limit Flow= 5% of Peak flow yes trigger Pressure limit Based on VT/C cycle off no Control logic for volume support mode of the servo 300
Dual Control Breath-to-Breathpressure-limited flow-cycled ventilationVolume Support • Little data to show it actually works. • If pressure support level increases to maintain TV in pt with increased airways resistance, PEEPi may increase. • If minimum TV set too high, weaning may be delayed.
VS (Volume Support) • Indications • Spontaneous breathing patient who require minimum E • Patients who have inspiratory effort who need adaptive support • Patients who are asynchronous with the ventilator • Used for patient who are ready to wean
VS (Volume Support) • Advantages • Guaranteed VT and E • Pressure supported breaths using the lowest required pressure • Decreases the patient’s spontaneous respiratory rate • Decreases patient WOB • Allows patient control of I:E time • Breath by breath analysis • Variable I to meet the patient’s demand
VS (Volume Support) • Disadvantages • Spontaneous ventilation required • VT selected may be too large or small for patient • Varying mean airway pressure • Auto-PEEP may affect proper functioning • A sudden increase in respiratory rate and demand may result in a decrease in ventilator support
Dual Control Breath-to-Breathpressure-limited time-cycled ventilationPressure Regulated Volume Control Maquet Servo-i Servo 300
Dual Control Breath-to-Breathpressure-limited time-cycled ventilationPressure Regulated Volume Control • Delivers patient or timed triggered, pressure-targeted (controlled) and time-cycled breaths • Ventilator measures VT delivered with VT set on the controls. If delivered VT is less or more, ventilator increases or decreases pressure delivered until set VT and delivered VT are equal
Dual Control Breath-to-Breathpressure-limited time-cycled ventilationPressure Regulated Volume Control • The ventilator will not allow delivered pressure to rise higher than 5 cm H2O below set upper pressure limit • Example:If upper pressure limit is set to 35 cm H2O and the ventilator requires more than 30 cm H2O to deliver a targeted VT of 500 mL, an alarm will sound alerting the clinician that too much pressure is being required to deliver set volume (may be due to bronchospasm, secretions, changes in CL, etc.)
PRVC (Pressure Regulated Volume Control) PRVC. (1), Test breath (5 cm H2O); (2) pressure is increased to deliver set volume; (3), maximum available pressure; (4), breath delivered at preset E, at preset f, and during preset TI; (5), when VT corresponds to set value, pressure remains constant; (6), if preset volume increases, pressure decreases; the ventilator continually monitors and adapts to the patient’s needs
yes Volume from Ventilator= Set tidal volume no calculate compliance Calculate new Pressure limit time= set Inspiratory time yes trigger Pressure limit Based on VT/C cycle off no Control logic for pressure-regulated volume control and autoflow
PRVC (Pressure Regulated Volume Control) • Disadvantages and Risks • Varying mean airway pressure • May cause or worsen auto-PEEP • When patient demand is increased, pressure level may diminish when support is needed • May be tolerated poorly in awake non-sedated patients • A sudden increase in respiratory rate and demand may result in a decrease in ventilator support
PRVC (Pressure Regulated Volume Control) • Indications • Patient who require the lowest possible pressure and a guaranteed consistent VT • ALI/ARDS • Patients requiring high and/or variable I • Patient with the possibility of CL or Raw changes
PRVC (Pressure Regulated Volume Control) • Advantages • Maintains a minimum PIP • Guaranteed VT and E • Patient has very little WOB requirement • Allows patient control of respiratory rate and E • Variable E to meet patient demand • Decelerating flow waveform for improved gas distribution • Breath by breath analysis
P aw cmH 0 2 A New Twist… Volume Targeted 60 SEC 1 2 3 4 5 6 -20 120 INSP Flow SEC 1 2 3 4 5 6 L/min 120 EXH Many Dual Modes start out looking like PCV
P aw cmH 0 2 Volume Targeted (Pressure Controlled) 60 SEC 1 2 3 4 5 6 -20 120 INSP Flow SEC 1 2 3 4 5 6 L/min 120 EXH As compliance changes - flow and volumes change
P aw cmH 0 2 New Volume Targeted Breath Pressure Variability is Controlled 60 SEC 1 2 3 4 5 6 -20 120 INSP Flow SEC 1 2 3 4 5 6 L/min 120 EXH Pressure then raises to assure that the set tidal volume is delivered
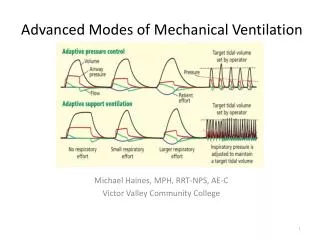
ASV (Adaptive Support Ventilation) • A dual control mode that uses pressure ventilation (both PC and PSV) to maintain a set minimum E (volume target) using the least required settings for minimal WOB depending on the patient’s condition and effort • It automatically adapts to patient demand by increasing or decreasing support, depending on the patient’s elastic and resistive loads
ASV (Adaptive Support Ventilation) • The clinician enters the patient’s IBW, which allows the ventilator’s algorithm to choose a requiredE. The ventilator then delivers 100 mL/min/kg. • A series of test breaths measures the system C, resistance and auto-PEEP • If no spontaneous effort occurs, the ventilator determines the appropriate respiratory rate, VT, and pressure limit delivered for the mandatory breaths • I:E ratio and TIof the mandatory breaths are continually being “optimized” by the ventilator to prevent auto-PEEP • If the patient begins having spontaneous breaths, the number of mandatory breaths decrease and the ventilator switches to PS at the same pressure level • Pressure limits for both mandatory and spontaneous breaths are always being automatically adjusted to meet the E target
ASV (Adaptive Support Ventilation) • Indications • Full or partial ventilatory support • Patients requiring a lowest possible PIP and a guaranteed VT • ALI/ARDS • Patient requiring high and/or variable • Patients not breathing spontaneously and not triggering the ventilator • Patient with the possibility of work land changes (CL and Raw) • Facilitates weaning
ASV (Adaptive Support Ventilation) • Advantages • Guaranteed VT and E • Minimal patient WOB • Ventilator adapts to the patient • Weaning is done automatically and continuously • Variable to meet patient demand • Decelerating flow waveform for improved gas distribution • Breath by breath analysis
ASV (Adaptive Support Ventilation) • Disadvantages and Risks • Inability to recognize and adjust to changes in alveolar VD • Possible respiratory muscle atrophy • Varying mean airway pressure • In patients with COPD, a longer TE may be required • A sudden increase in respiratory rate and demand may result in a decrease in ventilator support
Automode • The ventilator switch between mandatory and spontaneous breathing modes • Combines volume support (VS) and pressure-regulated volume control (PRVC) • If patient is paralyzed; the ventilator will provide PRVC. All breaths are mandatory that are ventilator triggered, pressure controlled and time cycled; the pressure is adjusted to maintain the set tidal volume. • If the patient breathes spontaneously for two consecutive breaths, the ventilator switches to VS. All breaths are patient triggered, pressure limited, and flow cycled. • If the patient becomes apneic for 12 seconds; the ventilator switches back to PRVC
MMV (Mandatory Minute Ventilation) • AKA: Minimum Minute Ventilation or Augmented minute ventilation • Operator sets a minimum E which usually is 70% - 90% of patient’s current E. The ventilator provides whatever part of the E that the patient is unable to accomplish. This accomplished by increasing the breath rate or the preset pressure. • It is a form of PSV where the PS level is not set, but rather variable according to the patient’s need
MMV (Mandatory Minute Ventilation) • Indications • Any patient who is spontaneously and is deemed ready to wean • Patients with unstable ventilatory drive • Advantages • Full to partial ventilatory support • Allows spontaneous ventilation with safety net • Patient’s E remains stable • Prevents hypoventilation
MMV (Mandatory Minute Ventilation) • Disadvantages • An adequate E may not equal sufficient A (e.g., rapid shallow breathing) • The high rate alarm must be set low enough to alert clinician of rapid shallow breathing • Variable mean airway pressure • An inadequate set E (>spontaneous E) can lead to inadequate support and patient fatigue • An excessive set E (>spontaneous E) with no spontaneous breathing can lead to total support