Download
1 / 80
810 likes | 847 Vues
DEGENERATIVE OSTEOARTHRITIS. Assoc. Prof. Ece AYDOĞ Physical Medicine and Rehabilitation. Learning objectives:. 1. be able to describe the pathogenesis of osteoarthritis 2. be able to enumerate the reasons of primer and secondary osteoarthritis

E N D
DEGENERATIVE OSTEOARTHRITIS Assoc. Prof. Ece AYDOĞ Physical Medicine and Rehabilitation
Learning objectives: 1. be able to describe the pathogenesis of osteoarthritis 2. be able to enumerate the reasons of primer and secondary osteoarthritis 3. be able to enumerate risk factors for osteoarthritis 4. be able to enumerate clinical and radiographic features of osteoarthritis (espc. knee, hip, hand) 5. be able to enumerate approaches to diagnosis and treatment of osteoarthritis
Structural classification is based on the materials that hold the joint together and whether or not a cavity is present in the joint. There are three structural classes.
Fibrous joints are held together by fibrous connective tissue. No joint cavity is present. Fibrous joints may be immovable or slightly movable. • Cartilaginous joints are held together by cartilage (hyaline or fibrocartilage). No joint cavity is present. Cartilaginous joints may be immovable or slightly movable. • Synovial joints are characterized by a synovial cavity (joint cavity) containing synovial fluid. Synovial joints are freely movable and characterize most joints of the body.
Functional Classification -is based on the degree to which the joint permits movement. There are three types: • A synarthrosis joint permits no movement. Structurally, it may be a fibrous or cartilaginous joint. • An amphiarthrosis joint permits only slight movement. Structurally, it may be fibrous or cartilaginous joint. • A diarthrosis joint is a freely movable joint. Structurally, it is always a synovial joint.
OSTEOARTHRITISOA "Osteoarthritis" is derived from the Greek word "osteo", meaning "of the bone", "arthro”, meaning "joint", and "itis", meaning inflammation, although many sufferers have little or no inflammation.
Synonyms • Degenerative joint disease • Arthrosis • Osteoarthrosis • Hypertrophic arthritis • Degenerative arthritis
Osteoarthritis is a type of arthritis that is caused by the breakdown and eventual loss of thecartilage of one or more joints. Cartilage is a protein substance that serves as a "cushion" between the bones of the joints.
Constituents of hyaline cartilage • Chondrocytes • Matrix (extracellular material) – Collagen fibres – Proteoglycan molecules
Cartilage is an avascular connective tissue which is composed of two elements:cellular component (5%) - the chondrocytesextracellular component(95%) - the matrix Water comprises approximately 70% of the matrix, the remainder consists primarily of collagen (especially collagen II) which is meshed with proteoglycanaggregates. .
• Large hygroscopic molecules • Long central chain of hyaluronic acid • Numerous side chains alongs its length, each with – Central cores of protein – Chondroitin sulphate and keratan sulphate side chains • Pg’s attract water and put collagen under tension Proteoglycan Aggregate
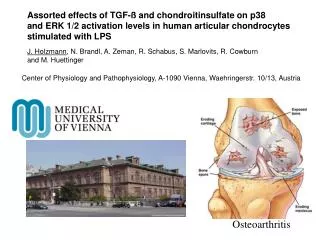
The swelling pressure of the fully hydrated but compressed aggrecans is counterbalanced by the tight collagen network. Due to this unique composite structure, healthy articular cartilage can resist major pressure and shear forces Normal Articular Cartilage
Rupture of collagen fibres, the protein makeup of cartilage degenerates More water is absorbed by proteoglycans Cartilage is considerably weakened Softening and swelling of cartilage
Fibrillation and cracks – Fine flakes of superficial cartilage become loosened and flake off (and cause mild secondary synovitis which can lead to ‘cold’ effusions) – Cracks appear in cartilage: eventually run through full thickness of cartilage
– Progressive loss of cartilage – Ultimate loss of full thickness of cartilage – Exposed bone becomes very hard with a polished appearance: ‘eburnation’ of bone (looks like ivory) Erosion of cartilage and eburnation
Synovial effusions: small and “cold” Subchondral cysts: Fluid is forced through clefts in cartilage into the underlying bone, can seen on X-ray Synovitis
Osteoblastic stimulation (repair attempt)– Underneath the damaged cartilage: subchondralsclerosis on X-ray– Around edge of joint forming lip of bone: fibroosseusosteophytes
Summary • Softening and swelling • Fibrillation • Full thickness cracks • Eburnation • Subchondral cysts • Subchondral sclerosis • Osteophyte formation
Epidemyology • Most common disease of joints over age 65 • Radiologically correlates poorly with symptoms • Rapid increase in radiologic evidence of OA after age 40 • Before age 45, osteoarthritis occurs more frequently in males. After age 55 years, it occurs more frequently in females.
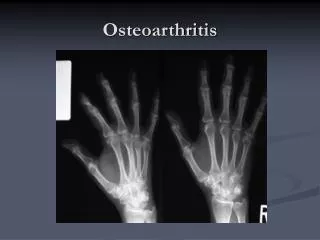
Osteoarthritis commonly affects the hands, feet, spine, and large weight-bearing joints, such as the hips and knees. • Most cases of osteoarthritis have no known cause : PRIMARY osteoarthritis. • When the cause is known, the condition is referred to as SECONDARY osteoarthritis.
Primary OA is mostly related but no caused by aging.
Secondary OA GeneticEndocrineMetabolic Anatomic Traumatic InflammatoryNeuropathic
Secondary OA Genetic: A genetic defect may promote breakdown of the protective architecture of cartilage. Ehlers-Danlos syndrome
Secondary OA Endocrine: • DM, • Acromegaly, • Hypotroidism, • Hypertroidism, • Obesity. Metabolic: • Paget disease • Wilson disease
Secondary OA Congenitalor developmental: Abnormal anatomy such as unequal leg length may be a cause of osteoarthritis. Posttraumatic: Macrotrauma or microtrauma. -Microtrauma may occur over time (chronically). An example of this would be repetitive movements or the overuse noted in several occupations.
Secondary OA Inflammatoryjoint diseases: This category would include infected joints, chronic gouty arthritis, and rheumatoid disease. Neuropathic: Diseases such as diabetes can cause nerve problems. The loss of sensation may affect how the body knows the position and condition of the joints or limbs. In other words, the body can't tell when it is injured.
Secondary OA Others: Nutritional problems Hemophilia Sickle cell anemia
Individual risk factors fordevelopment of OA • Obesity: knee > Hip • Family history (genetic): polyarticular esp hands • Trauma • Hypermobility • Dysplasia: Hip and knee • Occupation and sport: excessive and repeated loading of a joint
Clinical features Pain and tenderness • Originates in joint /periarticular soft tissue • Diffuse/ sharp and stabbing local pain • Initially, symptomatic patients incur pain during activity, which can be relieved by rest and may respond to simple analgesics. • Joints may become unstable as the OA progresses; therefore, the pain may become more prominent (even during rest) and may not respond to medications. Morning joint stiffnessusually lasts for less than 30 minutes.
PAİN • Sources of pain in osteoarthritis include the following: • Joint effusion and stretching of the joint capsule • Increased vascular pressure in subchondral bone • Torn menisci • Inflammation of periarticular bursae • Periarticular muscle spasm • Psychological factors • Crepitus (a rough or crunchy sensation) may be palpated during motion of an involved joint.
Types of pain • Mechanical: • Increases with use of the joint • Inflammatory: • Rest pain later on in 50% • Night pain in 30% later on
Movement abnormalities • “Gelling”: stiffness after periods of inactivity ;Passes over within minutes of using joint again • Coarse crepitus: palpate/hear • Reduced ROM: capsular thickening and bony changes in joint.
Deformities • Mild synovitis • Osteophytes • Joint laxity • Asymmetrical joint destruction leading to angulation
Heberden’s nodes, large firm swellings some of which are tender and red due to associated inflammation of the periarticular tissues as well as the joint. Hand OADIP, PIP, CMC
OA of the knees can affect any combination of the three main compartments of each knee. It is usually asymmetrical, and the compartments most frequently involved are the medial tibiofemoral and patellofemoral compartments. KNEE OA
Mild varus angulation of the knee joints due to asymmetrical OA of the medial tibiofemoral compartments. KNEE OA