Download
1 / 50
510 likes | 1.04k Vues
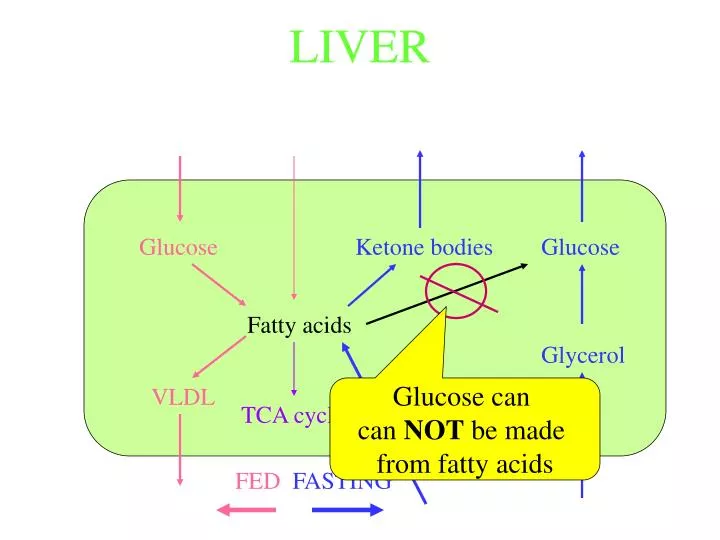
LIVER. Glucose. Ketone bodies. Glucose. Fatty acids. Glycerol. VLDL. Glucose can can NOT be made from fatty acids. TCA cycle. FED FASTING. Roles of Various Tissues in TG metabolism: MUSCLE. Glucose. Fatty acids. Ketone bodies. Glucose. Acetyl-CoA. Lactate (anaerobic).

E N D
LIVER Glucose Ketone bodies Glucose Fatty acids Glycerol VLDL Glucose can can NOT be made from fatty acids TCA cycle FED FASTING
Roles of Various Tissues in TG metabolism:MUSCLE Glucose Fatty acids Ketone bodies Glucose Acetyl-CoA Lactate (anaerobic) TCA cycle (aerobic) Not possible FED FASTING
Control by Hormone sensitive lipase Insulin mobilization VLDL Chylomicrons (liver) (intestine) L.P.Lipase Albumin Fatty acids Fatty acids Triacylglycerol Glucose Glycerol Control by GLUT-4 & L.P.Lipase Insulin uptake FED FASTING
PPAR • Increased PPAR activity increases the amount of many adipocyte proteins as well as proteins in other tissues. • Thiazolidinediones (TZDs) increase the sensitivity of tissues to the effects of insulin;Type II diabetics have decreased insulin sensitivity. • TZDs work by increasing the activity of PPAR • The exact reason for the increased insulin sensitivity is not clear.
INTESTINE Food & Bile salts Bile salts Pancreatic Lipase Fatty acids 2-Monoacylglycerol Other lipids Acly-CoA Triacylglycerol Apolipoprotein B-48 Chylomicrons Lymph
Chylomicron formation The process is analagous to VLDL formation in the liver BUT Apolipoprotien B-48 is used rather than Apolipoprotien B-100 Lipids are packaged as apolipoprotein B-48 is being synthesized: chylomicron From Shelness & Sellers (2001) Curr Opin Lipidology 12:151-157
Chylomicron formation • The same gene gives rise to both Apolipoprotien B-48 and Apolipoprotien B-100. • The mRNA for apoliprotein B-48 is derived from the apolipoprotein B-100 mRNA by tissue specific mRNA editing. • In intestinal cells an enzyme deaminates a specific cytidine nucleotide to Uridine. This highly specific C to U change introduces a stop codon, resulting in a shorter protein: apolipoprotein B-48 CAA B100 (made in liver) mRNA editing Stop codon UAA B48 (made in intestine)
BRAIN Fatty acids Glucose Glucose Ketone bodies Not metabolized Acetyl-CoA TCA cycle FED FASTING
Lipid Transport • Three Major Lipoprotein Pathways • Chylomicron pathway • Delivery of dietary lipid to tissues • VLDL • Delivery of lipid synthesized by liver to tissues • HDL • Cholesterol scavenger • Albumin • Transport of free fatty acids • Specialized Carriers • Some steroids • Some vitamins
Lipid Transport • The term lipoprotein refers to a particle that contains lipid plus apolipoprotein. • The term apolipoprotein refers to a protein without the associated lipid. • Example: VLDL is a lipoprotein, and apolipoprotein B-100 is a protein component of VLDL
Lipid Transport • Important core apolipoproteins • Apolipoprotein B-100 • Liver - formation of VLDL • Apolipoprotien B-48 • Intestine - formation of chylomicrons • A shortened version of apolipoprotein B-100 shortened through RNA editing • Apolipoproteins A-I and A-II • Central protein component of HDL • Made in Liver and intestine
Lipid Transport • Apolipoproteins added extra-cellularly • Apolipoproteins C-I, C-II, C-III • C-II is required for the activation of lipoprotein lipase • C-III ia an antagonist of lipoprotein lipase • C-I is a modulator of cholesterol exchange • Apolipoprotein E • Involved in recognition and uptake of lipoproteins by the liver • Three common alleles (E2, E3, E4) • E2/E2 is a risk factor for hyperlipoproteinemia • E4 is a risk factor for Alzheimer Disease
VLDL Liver Blood B-100 B-100 - Apolipoprotein B-100 TG - Triagylglycerol PL - Phospholipid Ch - Cholesterol ChE - Cholesterol ester TG PL, Ch, ChE VLDL Cholesterol Cholesterol ester
VLDL Liver Blood B-100 C TG PL, Ch, ChE HDL E VLDL B-100 TG PL, Ch, ChE E C
VLDL Liver Blood B-100 E n d o C t e h l e l l i a l M u s c l e C TG PL, Ch, ChE HDL E VLDL B-100 TG PL, Ch, ChE E C Adipose Fatty Acid + Glycerol Lipoprotein Lipase
VLDL Liver Blood B-100 E n d o C t e h l e l l i a l M u s c l e C TG PL, Ch, ChE HDL E VLDL B-100 B-100 TG,PL Ch, ChE TG PL, Ch, ChE E E C IDL Adipose C Fatty Acid + Glycerol HDL
VLDL Liver Blood B-100 E n d o C t e h l e l l i a l M u s c l e C TG PL, Ch, ChE HDL E VLDL B-100 B-100 IDL TG,PL Ch, ChE TG PL, Ch, ChE E E C Adipose C ChE Fatty Acid + Glycerol B-100 HDL TG,PL Ch, ChE E LDL
VLDL Liver Blood B-100 E n d o C t e h l e l l i a l M u s c l e C TG PL, Ch, ChE HDL E VLDL B-100 B-100 IDL TG,PL Ch, ChE TG PL, Ch, ChE E E LDL Receptor C Adipose LDL C ChE Fatty Acid + Glycerol B-100 HDL TG,PL Ch, ChE Lysosomal degredation E ChE Ch F.A. A.A. Most cells have LDL receptors Liver Bile salts
LDL Receptor B-100 TG,PL Ch, ChE VLDL Liver Blood B-100 E n d o C t e h l e l l i a l M u s c l e E C TG PL, Ch, ChE HDL E VLDL B-100 E B-100 IDL TG,PL Ch, ChE TG,PL Ch, ChE TG PL, Ch, ChE E B-100 E LDL Receptor C Adipose LDL C ChE Fatty Acid + Glycerol B-100 HDL TG,PL Ch, ChE Lysosomal degredation E ChE Ch F.A. A.A. Most cells have LDL receptors Liver Bile salts
Intracellular Cholesterol Metabolism LDL receptor LDL
Intracellular Cholesterol Metabolism Lysosome LDL
Intracellular Cholesterol Metabolism Lysosome Amino acids LDL Fatty acids + Glycerol Cholesterol
Liver Cholesterol Metabolism LDL, chylomicron remnants VLDL HMG-CoA reductase HMG-CoA Cholesterol Acyl-CoA 19.5 grams/day Bile salts Cholesterol ester 20 grams/day 0.5 grams/day Bile
Liver Cholesterol Metabolism Inhibition of HMG-CoA reductace and Bile salt readsorption are important therapeutic targets. VLDL Cholesterol inhibits Transcription DNA HMG-CoA reductase Acyl-CoA HMG-CoA Cholesterol Bile salts Cholesterol ester
Periperal Cholesterol Metabolism Tangier Disease: a lack of ABC-A1 HDL Ch to HDL Inhibition of HMG-CoA reductace is an important therapeutic target. ABC-A1 transporter Cholesterol inhibits Transcription DNA HMG-CoA reductase HMG-CoA Cholesterol Cholesterol ester
- NORMAL FAMILIAL HYPERCHOLESTEROLEMIA Remains in blood To blood To blood LDL LDL LDL LDL receptor LDL Lysozyme LDL LDL receptor Lysozyme Cholesterol export LDL Lysozyme LDL receptor Cholesterol export LDL LDL receptor Cholesterol LDL LDL receptor De novo Cholesterol synthesis Cholesterol Nucleus LDL Nucleus LDL receptor LDL Remains in blood Cholesterol synthesis is limited Cholesterol synthesis is not as limited
Chylomicrons Intestine Lymph B-48 B-48 - Apolipoprotein B-48 TG - Triagylglycerol PL - Phospholipid Ch - Cholesterol ChE - Cholesterol ester TG PL, Ch, ChE Chylomicron Cholesterol Cholesterol ester
Chylomicrons Intestine Lymph Blood B-48 HDL C TG PL, Ch, ChE E B-48 TG PL, Ch, ChE E C
Chylomicrons E n d o C t e h l e l l i a l Intestine Lymph Blood M u s c l e B-48 HDL C TG PL, Ch, ChE E B-48 TG PL, Ch, ChE E C Adipose Fatty Acid + Glycerol Lipoprotein Lipase
Chylomicrons E n d o C t e h l e l l i a l Intestine Lymph Blood M u s c l e B-48 HDL C TG PL, Ch, ChE E B-48 Chylomicron TG PL, Ch, ChE E C Adipose B-48 Fatty Acid + Glycerol TG,PL Ch, ChE C E HDL Chylomicron Remnant
Chylomicrons E n d o C t e h l e l l i a l Intestine Lymph Blood M u s c l e B-48 HDL C TG PL, Ch, ChE E B-48 TG PL, Ch, ChE E C Adipose B-48 Fatty Acid + Glycerol TG,PL Ch, ChE C E HDL LRP (LDL receptor-related protein) Liver
Chylomicrons E n d o C t e h l e l l i a l Intestine Lymph Blood M u s c l e B-48 HDL C TG PL, Ch, ChE E B-48 TG PL, Ch, ChE E C Adipose B-48 Fatty Acid + Glycerol TG,PL Ch, ChE C E Lysosomal degradation HDL ChE Ch F.A. A.A. LRP (LDL receptor-related protein) Liver Bile salts
HDL Intestine Lymph Blood PL,Ch A Liver
T I S S U E HDL Intestine Lymph Blood LDL PL,Ch A B-100 TG,PL Ch, ChE E Ch ABC-A1 transporter ChE Liver
T I S S U E HDL Intestine Lymph Blood PL,Ch A Lecithin:cholesterol acyl transferase B-100 E C Ch PL,ChE A LCAT Ch ABC-A1 transporter ChE Tangier Disease: a lack of ABC-A1 Liver
HDL Intestine Lymph Blood A PL,Ch E C PL,ChE, TG LCAT A CETP Cholesterol ester transfer protein ChE TG TG, PL Ch, ChE E B-100 Liver
HDL Intestine Lymph Blood PL,Ch A E C PL,ChE, TG A LCAT CETP Hepatic Lipase H.L. F.A. + Glycerol TG,PL Ch, ChE E B-100 Liver
HDL Intestine Lymph Blood PL,Ch A E C PL,ChE A LCAT CETP H.L. SR-B-1 (Scavenger Receptor) Liver
Macrophages to “foam cells” Oxidized LDL (not recognized by LDL receptor) Export is limited B-100 TG,PL Ch, ChE SR-A (Scavenger Receptor A) E ABC-A-1 transporter Cholesterol Intracellular accumulation leading to “foam cell” (atherogenic)
Disorders of Lipid metabolism Type I diabetes: Very low insulin: cells act as if starving even though blood glucose is high. • Adipose: • Fatty acid mobilization up • Triacylglycerol synthesis is down • Liver: • Fatty acid synthesis is down (low glycolysis; low citrate) yet VLDL production is up. • Fatty acid oxidation is up • Ketone body formation is up: severe ketosis • Excess fatty acids go to VLDL formation: high blood lipid.
Dyslipidemias • Hypercholesterolemia • High LDL cholesterol • Hypertirgliceridemia • High blood triglycerides • Combined hyperlipidemia • High blood triglycerides and cholesterol • Hypoalphalipoproteinemia • Low HDL • Hypobetalipoproteinemia • Low VLDL & chylomicrons
Disorders of Lipid metabolism Type II diabetes: • Cells have a greatly reduced sensitivity to the effects of insulin • Molecular basis is poorly understood • Numerous hormones produced by adipocytes may play a role • Effects of obesity • PPAR modulates expression of important proteins
Disorders of Lipid metabolism Atheroschlerosis Important risk factors include: • High LDL/ HDL ratio • High concentration of small dense LDL particles • not efficiently taken up by liver • targets for oxidation • taken up by macrophage • Uptake of oxidized lipids by macrophages • Cholesterol processing by macrophages
Predisposing alleles and therapeutic targets: • Apolipoprotein B • VLDL/chylomicron metabolism • Apolipoproteins CII & CIII • rate of clearance of VLDL • Lipoprotein Lipase • Rate of clearance of VLDL • Apolipoprotein E • uptake of chylomicron remnants; LDL uptake • Three common Alleles • E2/E2 risk factor for hyperlipidemia • E4 risk factor for Alzheimer
Predisposing alleles and therapeutic targets: • LDL receptor • Rate of clearance of LDL • Familial hypercholesteolemia • Apolipoprotein A1 • low HDL • Cholesterol ester transfer protein (CETP) • HDL stability; LDL metabolism • ABC-A1 protein • Cholesterol export from cells, particularly macrophage • PPARαPPARγPPARδ









![[EPUB] DOWNLOAD Natural Liver Cleanse Recipes: Liver cleanse juices, liver cleanse tea, Liver cleanse soup, fatty liver](https://cdn7.slideserve.com/12507667/slide1-dt.jpg)