Download
1 / 48
480 likes | 640 Vues
CATCh. Community-based Adolescent Testing for Chlamydia at DERC. Objectives. Gain a better understanding of Sexually Transmitted Infections (STIs) with a specific focus on Chlamydia and Gonorrhea Discuss how STIs impact DJS youth and adolescents throughout the country

E N D
CATCh Community-based Adolescent Testing for Chlamydia at DERC
Objectives • Gain a better understanding of Sexually Transmitted Infections (STIs) with a specific focus on Chlamydia and Gonorrhea • Discuss how STIs impact DJS youth and adolescents throughout the country • Review the CATCh program model, materials, and plan for implementation • Discuss the role of DERC staff in the CATCh program
Do you know… • What are the most common STIs? • How STIs are transmitted? • Who is most at risk for STIs? • How to prevent STIs? • How to treat STIs? • What can happen if you don’t treat STIs?
Bacterial Chlamydia Gonorrhea Syphilis Parasitic Trichomoniasis (Trich) Pubic Lice Viral Herpes Simplex (HSV) 1 and 2 Hepatitis B/C HIV/AIDS HPV Molluscum Contagiosum What are the most common STIs?
How are STIs Transmitted? • Contact with infected body fluids such as vaginal secretions, semen, and blood • Skin to skin contact with an infected person during vaginal, anal, or oral sex • From mother to child • Some are curable (bacterial and parasitic) • others cannot be cured but can be treated (viral- HIV/Hepatitis) • May or may not have symptoms • Can affect areas other than the genitals (ie: eye, mouth, throat)
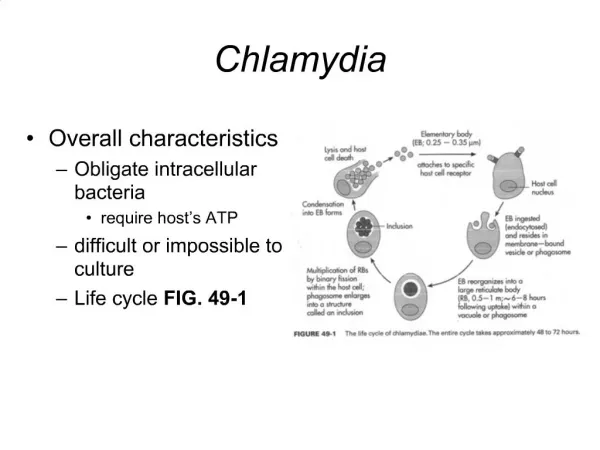
Chlamydia and Gonorrhea(CT & GC) • Most commonly reported STIs • In the U.S. in 2008, there were over 1.5 million cases of CT and GC reported to CDC (CDC, 2009). • Both are caused by bacteria • Chlamydia trachomatis • Neisseria gonorrhoeae • Both are can be treated with antibiotics • Urine test to detect presence of CT/GC
Chlamydia symptoms • 70% of females and 50% of males have NO SYMPTOMS! • Symptoms for women may include: • Unusual vaginal discharge • Pain or a burning sensation with urination • Bleeding between periods • Pain during sex or bleeding after sex • Low abdominal pain sometimes with nausea • Rectal pain, discharge or bleeding (w/ anal sex)
Chlamydia symptoms cont’d. • Symptoms for men may include: • White/cloudy, watery discharge from the tip of the penis • Pain or a burning sensation with urination • Testicular pain and/or swelling • Rectal pain, discharge or bleeding (w/ anal sex)
Gonorrhea symptoms • Most infections have NO SYMPTOMS! • Symptoms can include: • Burning with urination • White, yellow, or green discharge from the penis/vagina • Bleeding between periods • Sore throat – oral sex • Rectal pain or discharge
Treatment and Follow-up • Both treatable with antibiotics – several options • Antibiotic-resistant strains of gonorrhea are making treatment more challenging • Health teaching and prevention are crucial! • CONDOM USE • Risk reduction counseling – how are STIs spread and how to prevent • Emergency contraception • Family planning • Abstain from sex until treatment complete • Make sure partner is treated too • HIV testing/other STI testing
Why do we care? • If left untreated, CT & GC can lead to serious health consequences • In men • Painful inflammation of the epididymis (epididymitis) • Reduced fertility or sterility • In women – Pelvic Inflammatory Disease • Increased risk of ectopic pregnancy • Chronic pelvic pain • Early miscarriage or premature birth • Infertility • Perihepatitis (Fitz-Hugh Curtis syndrome)
Pelvic Inflammatory Disease • Infection of the upper reproductive tract • Causes damage to the uterus, ovaries, and fallopian tubes • Symptoms: lower abdominal pain, unusual vaginal discharge, fever, pain with urination and sex, irregular menstrual bleeding.
Consequences of PID • According to the CDC, over 750,000 women have an acute episode of PID each year • Over 75,000 women may become infertile as a result of PID • A large proportion of ectopic pregnancies that occur each year are due to PID • PID may result in chronic pelvic pain • CDC, 2010
The Interplay Between STIs and HIV • The presence of HIV facilitates the acquisition of STIs, and vice versa. Also, those who are HIV + are more likely to spread HIV if they also have a STI • Why? • Increased viral shedding • Breaks in mucous membranes • Increased inflammatory response
Adolescents and STIs • 19 million new STIs occur each year in the U.S. • Almost half (48%) of these infections occur in 15-24 year olds • Why are adolescents at high risk for STIs? • Sexually active young girls more vulnerable due to cervical cells that are not fully matured • Adolescents are more likely to engage in high risk behaviors while using drugs or alcohol • Barriers to prevention services due to inability to pay, transportation, concerns about confidentiality
Trends in CT/GC Rates • CT Rates have been steadily rising over the years • Higher rates in adolescents versus other age groups • Higher rates among females • Disproportionate burden among African Americans – especially among females • Baltimore City disproportionately affected
Are DJS youth more at risk for STIs? • High prevalence of risk factors for pregnancy and STIs • Inconsistent condom use • Younger age of sexual debut • Multiple sexual partners • Over-representation of African American youth • High rates of sexual abuse/assault • Sex in exchange for money or drugs • Substance abuse • Mental health disorders
2009 DJS Chlamydia Rates • Overall, 8.5% of all youth tested in DJS facilities were positive for CT. • 16.9% of females were positive for CT • 17.2% of black, 16.1% of Hispanic, and 14% of white females tested were positive • 7.6% of males were positive for CT • 8.7% of black and 3.3% of Hispanic and 2.1% of white males tested were positive
2009 DJS Gonorrhea Rates • Overall, 1.5% of all DJS youth tested were positive for GC • 5.9% of females were positive for GC • 8.3% of black, 3.2% of Hispanic, and 1.8% of white females tested were positive for GC. • 1.0% of males were positive for GC • 1.3% of black, 0.5% of Hispanic, and 0% of white males tested were positive
Question • All youth in secure DJS facilities are tested for Chlamydia and gonorrhea…why can’t we do it in the community too? • Youth in the community are at an even greater risk for STIs than those in residential facilities since they continue to be sexually active.
CT/GC Testing for Community DJS Youth • NCC=National Chlamydia Coalition • $10,000 mini-grant • Goal: Fund applicants with innovative strategies to increase Chlamydia screening and follow-up care in local communities. • Length of grant: 1 year • Meeting with FIT and DERC staff in 2009 to gauge interest • DJS applied in January 2010 – was awarded in February to begin work on July 1, 2010
CATCh • Community-based • Adolescent • Testing for • Chlamydia
CATCh Program Highlights • Chlamydia (and Gonorrhea) screening AND treatment • Individual risk-reduction counseling • Referral to community resources for STI treatment, partner treatment, family planning, or other health resources as needed • Group health education
CATCh program sites • Baltimore City DJS youth under community supervision at two sites: • Males: Baltimore City Day and Evening Reporting Center (DERC) • Females: Baltimore City Female Intervention Team (FIT) unit
DERC • Since we have a health center already in place at DERC – we have an opportunity to do more than just CT/GC testing. • What are some other issues we can address with our youth? • Health care access in the community • General health care • Oral health • Immunizations • …and so much more!
CATCh vision at DERC • DERC program staff link youth to health services and STI screening with DJS nurse • Basic health and STI screening for DERC youth • Risk reduction counseling, health education, and condom availability by DERC program and nursing staff
DERC – Initial visit with RN • Each youth will receive a brief intake assessment with RN • Health history • Current health problems/issues • Current medications • Immunization status • CT/GC urine testing • HIV testing (optional) • RPR (Syphilis) testing (optional) • Referral to MD
Getting the results • Courier to state lab 2x per week • <2 week turn around for results • Youth will need to see RN once results are received from the State lab
Follow-Up visit with MD/RN • RN (Digna, Florence) or Dr. Bittrick (MD) • Disclosure of results and treatment if needed • Health teaching and counseling • Condom availability • Referral to community resources if needed • Partner treatment Rx (in some cases) • Reinforce importance of re-testing
Confidentiality • Very important for teen to feel that information shared during testing is confidential • They need to know who else may have access to the information and what will be done with the information • Reporting of positives to BCHD, per MD law • Youth records are confidential – only RN/MD involved in testing should be privy to this information
Consenting for self • Can youth can consent for STI testing services without a parent knowing? • YES!
Minor Consent Law of Maryland • A minor has the same capacity as an adult to consent to medical treatment if • married, • a parent of a child, or • if in the judgment of the attending physician, delaying treatment to obtain consent of another individual would adversely affect the life of health of the minor (emergency situations)
Minor Consent Law of Maryland • A minor has the same capacity as an adult to consent to • Treatment or advice about drug abuse or alcoholism • Treatment or advice about STDs • Treatment or advice about pregnancy or contraception other than sterilization • Physical examination and treatment after alleged sexual assault
Minor Consent Law of Maryland • A minor who is 16 years or older has the same capacity as an adult to consent to counseling, testing, and treatment for mental or emotional disorders
Confidentiality • When will confidentiality be broken? • Risk of harm to self or others • Suspicion of abuse • Other situations? • Pregnancy disclosure • STI disclosure
Role of DERC staff • We are all part of the CATCh team! • Work in collaboration with health staff to facilitate testing and education • Referral to RN (sick call box or verbal request) • Provide health literature and condoms • Participate and help to facilitate group health education • Provide community resources (health card) to youth
Group Health Education • Collaboration between teachers, direct care staff, nurses, HQ somatic health staff • Health videos • Ongoing: Organized groups w/ lessons on sexual health topics • Day- during school day • Evening – after school hours
“Goody bags” • Each youth will receive a goody bag with health literature and condoms on the day the urine is collected. • Condoms and brochures also available in DERC office • Direct care staff can also provide these to youth at any time
Survive Outside • Training for staff in September • 1:1 counseling session • Video group discussion • Making Proud Choices! curriculum
Potential Challenges • Youth buy in and interest in screening and follow-up • Documenting & communicating screening & treatment • Ensuring confidentiality • Establishing and maintaining consistent group health education • Resource issues: staffing
Conclusion • Adolescents, particularly DJS youth are at high risk for STIs • CATCh is an exciting opportunity to prevent and treat STIs among DJS youth, and create resource linkages to the communities in which they live • In addition to CT/GC testing, CATCh provides an opportunity to connect youth with needed health services
Other questions? • Dr. Jennifer Maehr, DJS Medical Director • (410)230-3217 • maehrj@djs.state.md.us • Jessica Burns, DJS Nurse Consultant • (410)230-3387 • burnsj@djs.state.md.us