Download
1 / 34
830 likes | 2.36k Vues
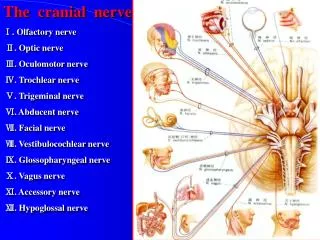
Optic Nerve Disease. Kelli Shaon, O.D. Congenital Optic Nerve Abnormalities. Morning Glory Disc. Unilateral, Larger nerve head Funnel shaped nerve head surrounded by chorioretinal pigment changes Vessels of the nerve head often appear hidden by glial tissue centrally

E N D
Optic Nerve Disease Kelli Shaon, O.D.
Morning Glory Disc • Unilateral, Larger nerve head • Funnel shaped nerve head surrounded by chorioretinal pigment changes • Vessels of the nerve head often appear hidden by glial tissue centrally • **Strong association with non-rhegmatogenous RD
Optic nerve head Coloboma • Unilateral, larger affected nerve • Often has unusual vascular pattern • Is the absence of tissue (retina, choroid, &/or ON) • Usually inferior portion ON • Vision varies (depends on severity) & VF defects vary (but are often dramatic) • **Strong association with non-rhegmatogenous RD
Optic Pit • Often appear as greenish-gray discoloration in area of ONH • Often inferior temporal (due to incomplete fetal fissure) • VF defects present that corresponds with pit location • **High Risk of Macular Serous Detachments
Optic Nerve Hypoplasia • Often unilateral but can be bilateral • Nerve head is typically 1/2 to 1/3 normal size • ON often surrounded by yellowish (or pigmented) zone – that would equal the size of the normal nerve • Called Double-ring sign • Vision if often decreased, & nystagmus can be present (due to ↓ VA since birth) • Strong association with systemic abnormalities (especially if bilateral)
Megalopapilla • Term used to describe larger ON when compared to fellow nerve • Diagnosis of exclusion (have to r/o of abnormalities) • Often has a larger C/D ratio
Optic Nerve drusen • Present in 1% of population • Higher incidence in Caucasians • Calcified hyaline bodies that are anterior to the lamina cribosa • In younger pts (children) can appear to be papilledema-like (no cupping), then with age appear to be yellowish, bumpy spherical retractile bodies superficial in ON • The deposits can cause interruption of axoplasmic flow which then may lead to VF defects that are known to progress • Deposits may also shear blood vessels causing hemorrhages which can affect vision
Optic Nerve drusen • Can autofluorescence w/ red-free filter • Hyperfluorescence on FA • Can interrupt axoplasmic flow, and interfere w/ vision & cause VF defects • Demonstrate highly reflective on ultrasound (B scan) • If extremely large drusen, can show up on CT
Common Benign Conditions • Pre-papillary Loop – thought to be an embryonic vessel • Ascends from the disc back to the disc • Projects into the vitreous & may move w/ eye movements • Cilioretinal Artery – derived from short posterior ciliary circulation • Occur in ~20% of individuals • Appears to start at temporal edge of disc & extend to macula • Supply inner retina & papillomacular bundle • Myelinated Nerve Fibers • Continuation of myelinated tissue anterior to the lamina • Appears as feathery superficial retinal opacification • May cause some VF depression
Common Benign Conditions • Tilted Discs – usually inferior-nasal tilt • Malinsertion syndrome - is tilted temporally (nasal disc is slightly elevated)
Leber’s hereditary Optic Atrophy • Bilateral • Acute presentation of rapid visual loss of 1 eye followed by the other eye within days or weeks • Average age of those affected 24 yo • Men>> Women (6.7 to 1) • Inherited by a mitochondrial DNA - (need genetic counseling) • Not transmitted by males • Transmitted (in carrier state) by females to 100% of daughters • Transmitted by females to manifest in 50% of sons • Transmitted by females to manifest in 10% of daughters
Leber’s hereditary Optic Atrophy • Presentation: • Acute onset: optic disc edema with accompanied small telangiectatic vessels near the disc (do not leak on IVFA) • Later stage: Followed by Severe optic atrophy • Visual acuity of 20/200 or worse & cecocentral VF defects • Management: • Genetic counseling • Low vision examination
Optic Neuritis (Papillitis) • Refers to “inflammation” of the optic nerve • Helpful to categorize optic neuritis as one of the following: • (1) Inflammatory-infectious (viral or bacterial) • (2) Demylinizing (multiple sclerosis) • (3) Idiopathic • Optic neuritis is most often associated with MS • If inflammatory or infectious – more likely to have swollen disc (ophthalmoscopy signs)
Optic Neuritis 2° to MS • Symptoms/Signs: • Unilateral loss of vision over hours to days • Pain is often associated with eye movement • If retrobulbar, no ophthalmoscopy signs may be seen – “Patient sees nothing and doctor sees nothing” • Decreased color perception – desaturation of “Red Cap” • Pulfrich phenomenon (altered perception of moving objects) • Increased symptoms with increased body temperature (most notable after hot shower or exercise) – Uhtoff’s sign • (+) APD • VF defects – central, cecocentral, arcuate or altitudinal
Optic Neuritis 2° to MS • Observations: • Optic nerve appears normal (retrobulbar) in 2/3 of cases • Optic nerve swelling is present in 1/3 of cases • Optic nerve head swelling does NOT correlate with severity of ON dysfunction • Flame shaped hemorrhages may be seen, but uncommon
Optic Neuritis 2° to MS • Management/Treatment: • Referral to a neurologist • MRI – often shows plaques formation • Presence of 1 or more plaques – 56% will develop CSMS • No plaques – 22% will develop MS • Steroids? Vs. Interferon therapy vs. No treatment • Outcome: • ~90% of pts will have visual recovery to 20/40 better within a few weeks • Recovery nearly complete by 5 weeks after episode
Optic Neuritis Treatment Trial • Used 3 treatment groups for Isolated Optic Neuritis: • IV methyprednisolone x3d, followed by PO prednisone taper • PO prednisone • Oral placebo for 14 days • Outcome: • At 6 months, visual recovery was the same for all 3 groups • 5 year follow-up : showed 87% of pts were 20/25 or better (despite treatment) • ** However, the ONTT demonstrated the use of PO steroids was associated with an increased risk of recurrent optic neuritis – DON’T USE PO STEROIDS ALONE • So Tx can be IV steroids, with PO taper OR no treatment
Controlled High Risk Avonex Multiple Sclerosis Prevention Study (CHAMPS): • Eligibility criteria: • Abnormal MRI – 2 or more lesions (min of 3 mm) • First neurological event (including optic neuritis) • Treatment groups: • Interferon-beta-1a (Avenox) – weekly IM injection followed by IV steroid x3d, then PO steroid 11 days • Weekly placebo IM injection followed by IV steroid x3d, then PO steroid 11 days • Results: • Avonex had a 44% reduction on the 3 year risk of CSMS when compared to placebo
Papilledema • Def: Optic disc edema produced by increased intracranial pressure • Symptoms/Signs: • Acute onset: • Bilateral (may be asymmetric) optic disc edema & hyperemia • Loss of SVP • Blurring of disc margins often obscuring disc vessels • NFL is often opacified • Disc hemes or CWS • Chronic papilledema • Resolution of hemes/CWS • Optic atrophy • Optociliary shunt vessels may develop • Transient visual disturbances, often w/ postural changes – lasting seconds • Headache • Enlarged Blind spot of VF testing – may expanded with time
Papilledema • Differential Diagnosis: • Long list – see Will’s for details • Work-up: • MRI/CT scan – to determine if space occupying lesion (tumor) • Lumbar puncture (LP), if CT or MRI does not reveal cause • Treatment: • Treat cause of increased ICP
Papillits vs. Papilledema • Papillitis is differentiated from papilledema • Unilateral instead of bilateral • Shows less elevation of the nerve head, and sluggish pupillary response • Will you get a APD with papilledema or a ↓ in color vision? • Not usually (rare exception - in chronic cases) but will in papillitis • When is the one exception when you can have unilateral “papilledema”? • Foster-Kennedy Syndrome is characterized by papilledema in one eye and optic atrophy in the other – This results from simultaneous raised ICP and optic nerve compression secondary to tumor
Pseudotumor Cerebri (PTC) • Symptoms/Signs: • Bilateral disc edema 2° to increased ICP (in the absence of space occupying lesion) • Headache (usually severe) – worse in the AM • Nausea &/or vomiting • Transient visual disturbances • Diplopia • Associated factors: • Female >>> male • Usually between 10-50 years of age • Obesity – ** Mnemonic – “Fat, Fertile, Female” • Pregnancy • Medications – (PO contraceptives, TCN, Vit A & PO steroid withdrawal)
Pseudotumor Cerebri (PTC) • Work-up: • MRI/CT scan to r/o tumor • LP - results often > 200 mm of water • Treatment: • Weight loss – if associated • Acetazolamide – Diamox PO 250 mg qid • Optic nerve decompression • Lumoperitoneal shunt
Ischemic Optic Neuropathy • Two types: • Non-artertic ischemic optic neuropathy (NAION) • Artertic ischemic optic neuropathy (AION) • They are NOT the Same – Must differentiate • After acute episode – 90% of AION will have cupping of the nerve compared to only 2% of NAION
Artertic Ischemic Optic Neuropathy(AION) • Etiology: Giant Cell Arteritis (GCA) • ***Ocular emergency *** Vision loss can become bilateral within hours to days • Almost always affects those > 50yo (w/ a mean age of 70+ yo) • High incidence of morbidity &/or mortality associated with GCA • Need to notify PCP immediately
Artertic Ischemic Optic Neuropathy(AION) • Signs/Symptoms: • Sudden, painless loss of vision (amaurosis fugax) – often CF or worse • Diplopia • (+) APD • (+) Altitudinal VF defect • Pale Diffuse edematous disc • Disc hemes possible • CRAO also possible (may be presenting sign) • Weight loss, fatigue, jaw claudication, temporal scalp tenderness, proximal muscle/joint pain (polymyalgia rheumatica), decreased temporal artery pulsation
Artertic Ischemic Optic Neuropathy(AION) • Work-up: • STAT Sed Rate (ESR) - Often extremely elevated • Normal: Male=(Age/2) Female= [(Age+10)/2] • C Reactive protein (CRP)– Often elevated • A elevated Sed rate & Elevated CRP = 97% specific for diagnosis of GCA • CBC w/ diff – often have anemia & thrombocytosis • Temporal artery biopsy – look for presence of arterial lumen damage & mononuclear cells • Treatment/Management: • No vision loss: PO steroids 60-100mg/day, taper • Acute Vision loss: Admit to hospital -- IV steroids (250mg q6h x12 doses), followed by PO steroids (slow taper)
Non-Artertic Ischemic Optic Neuropathy (NAION) • Etiology: Often vascular (Arteriosclerois, HTN, DM, anemia, and sleep apnea) • Thought to occur due to nocturnal hypotension • Often associated with a “disc at risk” – no/small physiologic cup • Diagnosis of exclusion- need to r/o of AION vs. other etiology
Non-Artertic Ischemic Optic Neuropathy (NAION) • Signs/Symptoms: • Sudden, painless loss of vision (amaurosis fugax) • Vision loss not usually as severe as in AION • (+) APD • (+) Altitudinal VF defect • Pale segmental swollen disc • Management/Treatment: • ESR, CRP, CBC w/ diff – to r/o out AION • Consider MRI/CT scan if compressive lesion is DDx • Measure blood pressure in office • Medical evaluation by internist or PCP • Follow-up 1 month or PRN based on severity
Compressive Optic Neuropathy • Signs/Symptoms: • Slowly progressive visual loss • (+) possible APD • VF defects – usually central • Proptosis • ON can be pale or swollen (varies) • Optociliary shunt vessels – vessels that shunt blood from the retina to the choroidal circulation)
Toxic/Nutritional Optic Neuropathy • Painless, progressive bilateral loss of vision • Bilateral cecocentral or central VF defects • Reduced color vision • Temporal disc pallor • Possible optic atrophy • Etiology: Alcohol, Malnutrition, B12 anemia (pernicious), other toxic substances • Work-up: History (alcohol or drug abuse, diet), B1, B12, Folate, CBC, heavy metal screening