Download
1 / 46
890 likes | 5.74k Vues
Applied Sciences Lecture Course. Short and Long term regulation of blood pressure. Mahesh Nirmalan MD FRCA PhD Consultant, Critical Care Medicine Manchester Royal Infirmary. A late response to blood loss is. Activation to chemo-receptors Release of Aldosterone from the adrenal gland

E N D
Applied Sciences Lecture Course Short and Long term regulation of blood pressure Mahesh Nirmalan MD FRCA PhD Consultant, Critical Care Medicine Manchester Royal Infirmary
A late response to blood loss is.. • Activation to chemo-receptors • Release of Aldosterone from the adrenal gland • Activation of baro-receptors • Sympathetic activation • Initiation of flight fright response
Vasomotor centre is located in the • Spinal cord • Pre-frontal cortex • Frontal cortex • Cerebellum • Brain stem
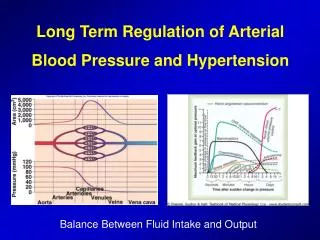
Local metabolic factors Calibre of the vessels Driving pressure & the pressure gradient Importance of mean arterial pressure Maintaining arterial pressure is a physiological imperative BP is maintained ……sometimes at the expense of regional blood flow Background: Tissue blood flow
Tissue blood flow is frequently independent of blood pressure: Auto-regulation
Blood pressure is a poor surrogate for tissue blood flow Serosal blood flow: sigmoid colon: pre aortic cross clamp MAP = 68 Serosal blood flow: sigmoid colon: post aortic cross clamp MAP = 90 MAP is a poor surrogate of tissue blood flow
Objectives • Physiology of arterial pressure • Short term regulation of blood pressure • Intermediate term • Long term regulation of blood pressure • Clinical examples • Vascular remodelling
Non-pulsatile flow in capillaries and veins Large pressure drop across the Arterioles: resistance vessels High pressure & pulsatile Blood Pressure = Cardiac Output x Total Peripheral Resistance V = I x R
Typical resistance arteriole post-ganglionic sympathetic neuron internal elastic lamina VSMC 10 µm endothelium From: Professor Arthur Weston, UoM
Aortic pressure Aortic flow
Arterial pressure is a product of a dynamic interplay between the force generated by the ventricles and the peripheral resistance vessels: Ventricular – vascular coupling
Rise of the blood pressure curve dependent on the characteristic Compliance of the Aorta Heart in systolic Phase Compliance Aortic valve open SV P(t)
Aortic compliance Diastole Fall of the blood pressure curve dependent on the characteristic Compliance of the Aorta Heart in diastolic Phase Aortic valve closed P(t) Rev Steven Hales: 1733; Otto Frank 1899
Arteriosclerosis increases the systolic pressure and lowers the diastolic pressure Nirmalan & Pinsky Year Book of ICEM 2010
Vasoconstriction:↑systolic & diastolic pressure Baseline 6 mg Ephedrine Post Ephedrine Nirmalan & Pinsky Year Book of ICEM 2010
Arterial pressure is a product of a dynamic interplay between the force generated by the ventricles and the peripheral resistance vessels:
Overview of systems Autonomic nervous system Fluid shifts Renal and endocrine responses
Stroke volume Vascular resistance Short term regulation of BP • Neurally mediated • Baro receptors, chemo receptors • Both arms of the ANS: sympathetic and parasympathetic • Ischaemic CNS response
Case study Diagnosis: Vasovagal syncope 20 year old medical student on the ward attempting venepuncture Suddenly looked pale, clammy and vacant Then vomited and collapsed with loss of consciousness Noted to have very slow, thready pulse Rapidly recovered
Gravity mediated increase in venous return Baro-receptor mediated vasoconstriction Restoration of SV and BP Return of consciousness Peripheral pooling Reduced venous return and stroke volume Reduced cerebral blood flow and syncope Stress relaxation of vessels Immediate and within seconds Involved in maintaining BP during ordinary physiological perturbations Powerful Hypovolaemic Shock Never complete Not sustainable
Effectors Afferent path ways Efferent pathways Centres Receptors
Baro-receptors • Nerve endings in all large thoracic and neck arteries • 2 major populations: Carotid sinus and Arch of the aorta • Activation on stretch • Carotid: Hering’s nerve to Glossopharyngeal nerve to tractus solitarius in brainstem • Aortic: Vagus nerve to tractus solitarius • If baro-receptors sense increased BP Secondary signals from tractus solitarius: Inhibition of vasoconstrictor centre and excitation of vagal parasympathetic centre
Baro-receptors • Important in maintaining postural blood pressure • (When standing from lying down strong sympathetic discharge) • Long term changes in blood pressure result in resetting of baroreflexes (i.e. not influential)
Case report Cardio-inhibitory Carotid Sinus Hypersensitivity 72 year old lady Collapsing in street, often when just about to cross road History of ischaemic heart disease and asthma Clinical examination unremarkable Postural blood pressures normal Referred for tilt table testing and carotid sinus massage
Chemo-receptors Sensitive to low O2, high CO2 and acidosis Chemoreceptor organs: 2 carotid bodies (one each bifurcation) 1-3 aortic bodies (adjacent to aorta) Separate blood supply Reduction in blood flow (reduction in pressure <80mmHg) causes metabolic stimulation Excitatory effect on vasomotor centre
Vasomotor centre: • Vasoconstrictor area • origin of excitatory pre-ganglionic vasoconstrictor neurones • Vasodilator area • internal inhibition of vasoconstrictor area • Sensory area • input from vagus and glossopharyngeal nerves modulate vasoconstrictor/dilator area activity
Anatomy of the autonomic nervous control of blood pressure: • Sympathetic vasomotor nerve fibres leave cord through (T+L) spinal nerves • Sympathetic chain • 1)Sympathetic nerves (viscera) • 2)Spinal nerves (vasculature) • Vagus nerve (PNS)
To raise the arterial pressure: • SNS release NA from nerve terminals • NA acts on the α adrenergic receptors of the VSMC • All arterioles constricted • Veins strongly constricted • Heart directly stimulated Not innervated: capillaries, precapillary sphincters and metarterioles
….It’s all about intracellular calcium VSMC Cardiovascular Physiology Concepts, Richard E Klabunde. www.cvphysiology.com
Beta-adrenoceptors Heart: Increased contractility Blood vessel: reduced contractility Cardiovascular Physiology Concepts, Richard E Klabunde. www.cvphysiology.com
The fluid shift is a continuous process • Changes in MAP will alter the pressure gradients • Net fluid shifts can be altered dramatically • Limited capacity Intermediate responses to changes in blood pressure • Within minutes • Starling forces at the level of the capillary bed • Redistribution of fluid within the vascular-interstitial compartments
Atrial volume reflex Reduced secretion of anti-diuretic hormone from hypothalamus Atrial stretch due to pressure Reflex dilation of renal afferent arteriole Reduction in water resorbtion from renal tubule Fluid loss by kidneys Increased glomerular capillary pressure Increased filtration of fluid into renal tubule
Long term control: The kidneys Pressure diuresis and pressure natriuresis Renin – Angiotensin- Aldosterone system Almost unlimited capacity Not a neural reflex Restores BP to precise limits
Pressure diuresis or pressure natriuresis A primitive adaptive system
Angiotensin II Flow rate in loop of Henle Macula Densa NaCL Glomerular Hydrostatic pressure Glomerular Filtration Pressure Na Cl resorption Arterial Pressure Renin Afferent arteriole Resistance GFR Efferent Arteriole Resistance
http://en.wikibooks.org/wiki/Human_Physiology/The_Urinary_Systemhttp://en.wikibooks.org/wiki/Human_Physiology/The_Urinary_System
Type II Diabetes and hypertension Essential Hypertension Increase in wall thickness Reduction in Lumen diameter Increase in wall to lumen ratio Preservation or mild impairment of endothelial function Increase in wall thickness No change/increase in lumen diameter Impairment of endothelial function Vascular Remodelling in common diseases Schofield, Circulation 2002;106:3037-43
Peri-vascular adipose tissue (PVAT) • Role in vascular tone?
Summary • Maintaining BP within a tight limit is a physiological imperative. • Immediate, Intermediate and delayed systems • Neural reflexes, fluid shifts and renal mechanisms • Age related changes to the vessel tone causes a gradual increase in BP as we age • Vascular remodelling: Hypertension, diabetes
Acknowledgements • Dr Adam Greenstein • Dr Reza Aghamohammadzadeh
??Supporting lecture on HypertensionProf A M Heagerty (Professor of Medicine, UoM): Available on-line