Download
1 / 4
40 likes | 187 Vues
Sandwich Infectious Keratitis (“SIK” Syndrome) – A New Clinical Entity Following Lamellar Keratoplasty (DLEK, DSAEK, DALK, ALK) T. John 1,2 , C. Karp 3 , E. Malbran 4 , L. Wiley 5 , M. John 2 , T. O’Brien 3 , J. Kieval 3 , R.K. Forster 3 , M. Gorovoy 6 , TE Gillette 7 , A. Panda 8 /

E N D
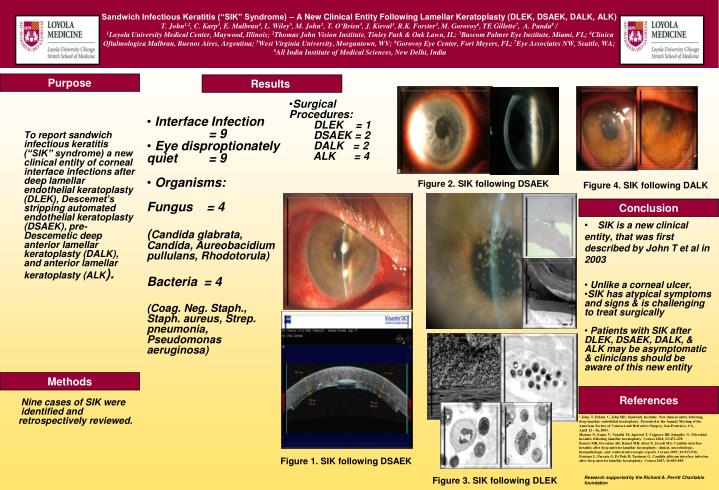
Sandwich Infectious Keratitis (“SIK” Syndrome) – A New Clinical Entity Following Lamellar Keratoplasty (DLEK, DSAEK, DALK, ALK) T. John1,2, C. Karp3, E. Malbran4, L. Wiley5, M. John2, T. O’Brien3, J. Kieval3, R.K. Forster3, M. Gorovoy6, TE Gillette7, A. Panda8 / 1Loyola University Medical Center, Maywood, Illinois; 2Thomas John Vision Institute, Tinley Park & Oak Lawn, IL; 3Bascom Palmer Eye Institute, Miami, FL; 4Clinica Oftalmologica Malbran, Buenos Aires, Argentina; 5West Virginia University, Morgantown, WV; 6Gorovoy Eye Center, Fort Meyers, FL; 7Eye Associates NW, Seattle, WA; 8All India Institute of Medical Sciences, New Delhi, India Purpose Results To report sandwich infectious keratitis (“SIK” syndrome) a new clinical entity of corneal interface infections after deep lamellar endothelial keratoplasty (DLEK), Descemet’s stripping automated endothelial keratoplasty (DSAEK), pre-Descemetic deep anterior lamellar keratoplasty (DALK), and anterior lamellar keratoplasty (ALK). • Interface Infection = 9 • Eye disproptionately quiet = 9 • Organisms: • Fungus = 4 • (Candida glabrata, Candida, Aureobacidium pullulans, Rhodotorula) • Bacteria = 4 • (Coag. Neg. Staph., Staph. aureus, Strep. pneumonia, Pseudomonas aeruginosa) • Surgical Procedures: DLEK = 1 DSAEK = 2 DALK = 2 ALK = 4 Figure 2. SIK following DSAEK Figure 4. SIK following DALK Conclusion • SIK is a new clinical entity, that was first described by John T et al in 2003 • Unlike a corneal ulcer, • SIK has atypical symptoms and signs & is challenging • to treat surgically • Patients with SIK after DLEK, DSAEK, DALK, & • ALK may be asymptomatic • & clinicians should be • aware of this new entity Methods References Nine cases of SIK were identified and retrospectively reviewed. • John, T, Delany C, John ME: Sandwich keratitis: New clinical entity following • deep lamellar endothelial keratoplasty. Presented at the Annual Meeting of the American Society of Cataract and Refractive Surgery, San Francisco, CA, • April 12 - 16, 2003. • Sharma N, Gupta V, Vanathi M, Agarwal T, Vajpayee RB, Satpathy G: Microbial keratitis following lamellar keratoplasty. Cornea 2004; 23:472-478. • Kanavi MR, Foroutan AR, Kamel MR, Afsar N, Javadi MA: Candida interface • keratitis after deep anterior lamellar keratoplasty: clinical, microbiologic, histopathologic, and confocal microscopic reports. Cornea 2007; 26:913-916. • Fontana L, Parente G, Di Pede B, Tassinari G: Candida albicans interface infection after deep anterior lamellar keratoplasty. Cornea 2007; 26:883-885. Figure 1. SIK following DSAEK Figure 3. SIK following DLEK Research supported by the Richard A. Perritt Charitable foundation
SIK: A New Clinical Entity Following Lamellar Keratoplasty (DLEK, DSAEK, DALK, ALK) • Purpose: • To report SIK a new clinical • entity of interface infectious • keratitis after DLEK, DSAEK, pre-Descemetic DALK, and ALK
Light and Electron Microscopic Analysis of Excised Human Descemet's Membrane Following Descemetorhexis with Endokeratoplasty E. B. Price1, T. John1, K.R. Kenyon2,3 1Loyola University Medical Center, Maywood, Illinois; 2Harvard Medical School, Boston, Massachusetts To measure the thickness of the DM, five photos were taken of each sample at 40x magnification and 10 thickness measurements were made on each photo using Scion Image software (Scion Corp., Frederick, MD). Visual excrescences scores were assigned as follows: 1 = smooth surface 2 = mild variability in sample thickness (1-3 excrescences per high-power-field [hpf]) 3 = moderate variability in sample thickness (4-6 excrescences per hpf) 4 = severe variability in sample thickness (>6 excrescences per hpf) the ranked mean (SD) of the excrescences samples (n = 15) was 3.33 (0.82), versus 1 (0) for the smooth samples (n = 13). This difference was also statistically significant (P < 0.01). Results Introduction Figure 4. Visual excrescences score in smooth and excrescences samples Light and electron microscopic examination of all samples revealed no residual corneal stroma. The mean (SD) thickness of the DM was 18.09 (6.99) µm in the patient group and 11.27 (2.90) µm in the normal controls, with no statistical difference between groups (P = 0.19). Patient samples with smooth DM had a mean (SD) thickness of 14.27 (2.70) µm, while those with DM excrescences averaged 21.40 (7.93) µm thick. This difference was statistically significant (P < 0.01). When the level of excrescences on the visual rating scale was compared between the two groups, Descemetorhexis with endokeratoplasty (DXEK, Descemet’s stripping automated endothelial keratoplasty, DSAEK) has become the treatment of choice for many types of corneal endothelial disease. A better understanding of the plane at which tissue separation occurs will promote the advancement of the best possible posterior lamellar keratoplasty technique. Figure 2. DM thickness in patients and controls Objective Smooth Excrescences Mean visual excrescences score in excised posterior lamellar tissue in smooth DM patient samples (n = 13) and sawtooth DM patient samples (n = 15). Bars indicate standard deviation. To evaluate the efficacy of descemetorhexis and Descemet’s stripping at producing a smooth recipient stromal surface in the context of descemetorhexis with endokeratoplasty. Table 1. Tissue characteristics Controls Patients Figure 1. Excised tissue samples Conclusion Mean thickness of Descemet’s membrane (DM) in excised posterior lamellar tissue in patients (n = 28) and controls (n = 2). Bars indicate standard deviation. Methods Descemetorhexis and Descemet’s stripping, performed in the present study with the John dexatome, produce a smooth separation of DM from the posterior stroma. As there was no recipient stromal loss, we presume the posterior stromal surface to be smooth. This information is encouraging because it reinforces that tissue separation occurs at the plane that we intend it to. Twenty-eight posterior lamellar recipient corneal samples were obtained from 27 DXEK patients through descemetorhexis and Descemet’s stripping with the John dexatome. Two samples from normal human donor eyes were also obtained as controls. All samples were examined using light microscopy and a representative sample was examined with transmission electron microscopy. All samples were evaluated for the presence of residual corneal stroma and the thickness of Descemet’s membrane (DM). Patient samples were also scored for the number of DM excrescences (guttata) per high power field. Figure 3. DM thickness in smooth and excrescences samples Insert Photo of Lenticules References Melles GRJ, Eggink FAGJ, Lander F, et al. A surgical technique for posterior lamellar keratoplasty. Cornea 1998;17:618.26. Melles GRJ, Wijdh RHJ, Nieuwendaal CP. A technique to excise the Descemet membrane from a recipient cornea (descemetorhexis). Cornea 2004;23:286.288. Melles GRJ, San Ong T, Ververs B, et al. Descemet membrane endothelial keratoplasty (DMEK). Cornea 2006;25:987.990. Tappin M. A method for true endothelial cell (Tencell) transplantation using a custom made cannula for the treatment of endothelial cell failure. Eye 2007;21:775.779. Melles GRJ, San Ong T, Ververs B, et al. Preliminary clinical results of Descemet membrane endothelial keratoplasty. Am J Ophthalmol 2008;145:222.227. Shimmura S, Miyashita H, Konomi K, et al. Transplantation of corneal endothelium with Descemet's membrane using a hyroxyethyl methacrylate polymer as a carrier. Br J Ophthalmol 2005;89:134.137. Ignacio TS, Nguyen TTB, Sarayba MA, et al. A technique to harvest Descemet's membrane with viable endothelial cells for selective transplantation. Am J Ophthalmol 2005;139:325.330. Terry MA, Hoar KL, Wall J, et al. Histology of dislocations in endothelial keratoplasty (DSEK and DLEK): a laboratory based, surgical solution to dislocation in 100 consecutive DSEK cases. 2006;25:926.932. Heindl LM, Hofmann-Rummelt C, Schlötzer-Schrehardt et al. Histologic analysis of Descemet stripping in posterior lamellar keratoplasty. Arch Ophthalmol. 2008;126:461.464. Tillet CW. Posterior lamellar keratoplasty. Am J Ophthalmol. 1956;41:530.533. Photo of all excised samples on light microscopy Smooth Excrescences Mean thickness of Descemet’s membrane (DM) in excised posterior lamellar tissue in smooth DM patient samples (n = 13) and excrescences DM patient samples (n = 15). Bars indicate standard deviation. Research supported by the Richard A. Perritt Charitable foundation
Light and Electron Microscopic Analysis of Excised Human Descemet's Membrane Following Descemetorhexis with Endokeratoplasty E. B. Price1, T. John1, K.R. Kenyon2,3 1Loyola University Medical Center, Maywood, Illinois; 2Harvard Medical School, Boston, Massachusetts To measure the thickness of the DM, Five photos were taken of each sample at 40x magnification and 10 thickness measurements were made on each photo using Scion Image software (Scion Corp., Frederick, MD). Visual excrescences scores were assigned as follows: 1 = smooth surface 2 = mild variability in sample thickness (1-3 excrescences per high-power-field [hpf]) 3 = moderate variability in sample thickness (4-6 excrescences per hpf) 4 = severe variability in sample thickness (>6 excrescences per hpf) the ranked mean (SD) of the excrescences samples (n = 15) was 3.33 (0.82), versus 1 (0) for the smooth samples (n = 13). This difference was also statistically significant (P < 0.01). Results Introduction Figure 4. Visual excrescences score in smooth and excrescences samples Light and electron microscopic examination of all samples revealed no residual corneal stroma. The mean (SD) thickness of the DM was 18.09 (6.99) mm in the patient group and 11.27 (2.90) mm in the normal controls, with no statistical difference between groups (P = 0.19). Patient samples with smooth DM had a mean (SD) thickness of 14.27 (2.70) mm, while those with DM excrescences averaged 21.40 (7.93) mm thick. This difference was statistically significant (P < 0.01). When the level of excrescences on the visual rating scale was compared between the two groups, Descemetorhexis with endokeratoplasty (DXEK, Descemet’s stripping automated endothelial keratoplasty, DSAEK) has become the treatment of choice for many types of corneal endothelial disease. A better understanding of the plane at which tissue separation occurs will promote the advancement of the best possible posterior lamellar keratoplasty technique. Figure 2. DM thickness in patients and controls Objective Smooth Excrescences Mean visual excrescences score in excised posterior lamellar tissue in smooth DM patient samples (n = 13) and sawtooth DM patient samples (n = 15). Bars indicate standard deviation. To evaluate the efficacy of descemetorhexis and Descemet’s stripping at producing a smooth recipient stromal surface in the context of descemetorhexis with endokeratoplasty. Table 1. Tissue characteristics Figure 1. Excised tissue samples Conclusion Controls Patients Mean thickness of Descemet’s membrane (DM) in excised posterior lamellar tissue in patients (n = 28) and controls (n = 2). Bars indicate standard deviation. Descemetorhexis and Descemet’s stripping, performed in the present study with the John dexatome, produce a smooth separation of DM from the posterior stroma. As there was no recipient stromal loss, we presume the posterior stromal surface to be smooth. This information is encouraging because it reinforces that tissue separation occurs at the plane that we intend it to. Methods Twenty-eight posterior lamellar recipient corneal samples were obtained from 27 DXEK patients through descemetorhexis and Descemet’s stripping with the John dexatome. Two samples from normal human donor eyes were also obtained as controls. All samples were examined using light microscopy and a representative sample was examined with transmission electron microscopy. All samples were evaluated for the presence of residual corneal stroma and the thickness of Descemet’s membrane (DM). Patient samples were also scored for the number of DM excrescences (guttata) per high power field. Figure 3. DM thickness in smooth and excrescences samples Insert Photo of Lenticules References Melles GRJ, Eggink FAGJ, Lander F, et al. A surgical technique for posterior lamellar keratoplasty. Cornea 1998;17:618.26. Melles GRJ, Wijdh RHJ, Nieuwendaal CP. A technique to excise the Descemet membrane from a recipient cornea (descemetorhexis). Cornea 2004;23:286.288. Melles GRJ, San Ong T, Ververs B, et al. Descemet membrane endothelial keratoplasty (DMEK). Cornea 2006;25:987.990. Tappin M. A method for true endothelial cell (Tencell) transplantation using a custom made cannula for the treatment of endothelial cell failure. Eye 2007;21:775.779. Melles GRJ, San Ong T, Ververs B, et al. Preliminary clinical results of Descemet membrane endothelial keratoplasty. Am J Ophthalmol 2008;145:222.227. Shimmura S, Miyashita H, Konomi K, et al. Transplantation of corneal endothelium with Descemet's membrane using a hyroxyethyl methacrylate polymer as a carrier. Br J Ophthalmol 2005;89:134.137. Ignacio TS, Nguyen TTB, Sarayba MA, et al. A technique to harvest Descemet's membrane with viable endothelial cells for selective transplantation. Am J Ophthalmol 2005;139:325.330. Terry MA, Hoar KL, Wall J, et al. Histology of dislocations in endothelial keratoplasty (DSEK and DLEK): a laboratory based, surgical solution to dislocation in 100 consecutive DSEK cases. 2006;25:926.932. Heindl LM, Hofmann-Rummelt C, Schlötzer-Schrehardt et al. Histologic analysis of Descemet stripping in posterior lamellar keratoplasty. Arch Ophthalmol. 2008;126:461.464. Tillet CW. Posterior lamellar keratoplasty. Am J Ophthalmol. 1956;41:530.533. Photo of all excised samples on light microscopy Smooth Excrescences Mean thickness of Descemet’s membrane (DM) in excised posterior lamellar tissue in smooth DM patient samples (n = 13) and excrescences DM patient samples (n = 15). Bars indicate standard deviation. Research supported by the Richard A. Perritt Charitable foundation



















