Download
1 / 32
350 likes | 608 Vues
Medtronic RDN SYMPLICITY HTN-3. Key Takeaways. SYMPLICITY HTN-3 did not reach the primary or powered secondary efficacy endpoints in this trial. There may be many factors that contributed to the outcome, which we continue to investigate .

E N D
Key Takeaways • SYMPLICITY HTN-3 did not reach the primary or powered secondary efficacy endpoints in this trial. There may be many factors that contributed to the outcome, which we continue to investigate. • SYMPLICITY HTN-3 did meet its safety endpoint, which is consistent with all other Symplicity trials, including the Global SYMPLICITY Registry. • Based upon our detailed analysis of HTN-3, we believe further clinical investigation is warranted and Medtronic will, in consultation with FDA, pursue a new IDE trial • An unmet need in this uncontrolled hypertension population still exists. Medtronic will continue to provide access to the Symplicity system in countries where it has regulatory approval and will continue to support a global hypertension clinical program
Trial Objectives • SYMPLICITY HTN-3 is the first prospective, multi-center, randomized, blinded, sham controlled study to evaluate both the safety and efficacy of percutaneous renal artery denervation in patients with severe treatment-resistant hypertension. • The trial included 535 patients enrolled by 88 participating US centers.
Key Inclusion/Exclusion Criteria Key Inclusion: • Stable medication regimen including full tolerated doses of 3+ anti hypertensive medications of different classes, including a diuretic • Office SBP ≥160 mm Hg based on an average of 3 blood pressure readings measured at both an initial and a confirmatory screening visit Key Exclusion: • ABPM 24 hour average SBP <135 mm Hg • eGFR of <45 mL/min/1.73 m2 • Main renal arteries <4 mm diameter or <20 mm treatable length
SYMPLICITY HTN-3: Severe Drug-Resistant HTN Office SBP ≥160 mm Hg • 2:1 randomization, blinded and controlled • Sham procedure in control patients that included renal angiogram • 535 subjects randomized out of 1441 enrolled (63% screen failure rate) • 2-week screening process, including maximum tolerated doses of antihypertensives 2 weeks 1 mo 3 mo 6mo Home BP & HTN med confirmation 2 weeks Home BP & HTN med confirmation Sham Procedure Renal angiogram; Eligible subjects randomized Primary endpoint Screening Visit 1 Screening Visit 2 • Office SBP ≥160 mm Hg • Full doses ≥3 meds • No med changes in past 2 weeks • No planned med changes for 6 mo • Office SBP ≥160 mm Hg • 24-h ABPM SBP≥135 mm Hg • Documented med adherence Renal Denervation Home BP & HTN med confirmation 2 weeks 6mo 1 mo 3mo 12-60 mo • Patients, BP assessors, and study personnel all blinded to treatment status • No changes in medications for 6 M
Key Safety Endpoint Safety analysis • Composite endpoint of death, renal injury, vascular complications, and embolic tissue injury to 1 month and renal artery stenosis to 6 months. <7% MAE rate required to meet the primary safety endpoint. Primary safety analysis • A performance goal established from renal artery stenting required the major adverse event rate for safety be <9.8%. This requires the observed MAE rate to be <7%, given the expected confidence interval for this endpoint.
Key Efficacy Endpoints Efficacy analysis • Comparison of SBP change from baseline to 6 mo in RDN arm compared with change from baseline to 6 mo in control arm • Endpoint = (SBPRDN 6 mo– SBPRDN baseline) – (SBPCTL: 6 mo– SBPCTL baseline) Primary efficacy (OBP) endpoint assumptions • Superiority analysis • Superiority margin of 5 mm Hg, per FDA recommendation • Assuming a standard deviation of 25 mm Hg for both arms, 10 mm Hg is the minimum treatment difference required to meet the efficacy endpoint (95% CI) Secondary efficacy (ABPM) endpoint assumptions • Superiority analysis • Superiority margin of 2 mm Hg, per FDA recommendation • Assuming a standard deviation of 18 for both arms, 5.5 mm Hg is the minimum difference required to meet the efficacy endpoint (95% CI)
Patient Disposition 1441 subjects assessed for eligibility • Excluded: • 880 not eligible for randomization • 26 eligible but not randomized because randomization cap was reached 535 subjects randomized 171 subjects randomly allocated to sham control 364 subjects randomly allocated to renal denervation 2:1 • 2 subjects died • 1 subject withdrew • 11 missed 6-month visit • 1 subject died • 1 missed 6-month visit 350 (96.2%) subjects with 6 month follow-up 169 (98.8%) subjects with 6 month follow-up
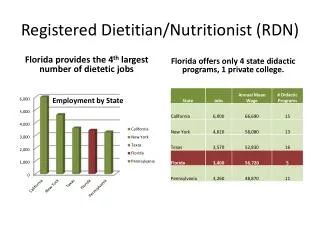
Results: Population Demographics *Race also includes Asian, Native American, or other
HTN-3 Results: Primary Safety Endpoint Performance Goal = 9.8% P < 0.001 Major Adverse Event (MAE) Rate
Primary Efficacy EndpointOffice Systolic Blood Pressure at 6 Months, 5 mm Superiority Margin N = 353 N = 171 ∆SBP at 6 mo -2.39 (-6.89, 2.12), P = 0.255 (Primary analysis with 5 mm Hg superiority margin) • Did not meet primary efficacy endpoint
Secondary Efficacy EndpointAmbulatory Systolic Blood Pressure at 6 Months, 2 mm Superiority Margin N = 325 N = 159 ∆ ABPM at 6 mo -1.96 (-4.97, 1.06), P = 0.979 (ITT analysis with 2 mm Hg superiority margin) • Did not meet secondary efficacy endpoint
HTN-3 Results: Potential Factors • Patient behavior • Due to being enrolled and closely monitored in a clinical trial, as well as blinded to treatment, the patients in SYMPLICITY HTN-3 may have improved or modified their lifestyle and drug adherence. • Study population • The population studied and the requirement for maximum tolerated medication dosage were different from other SYMPLICITY studies. • Procedural experience and variability • SYMPLICITY HTN-3 included a greater number of trial sites and proceduralists compared to SYMPLICITY HTN-1 and HTN-2, which may have led to greater procedural variability. • Case proctoring was different and not comparable
HTN-3: Challenge of Limiting Medication Changes in Uncontrolled Hypertension Population • Protocol mandated maximum doses and nomedication changes • ~40% of patients(n = 211) in the trial required medication changes • 69% of first medication changes were medically necessary Patients With Medication Changes (%) N = 71 N = 137
CHALLENGES OF SHAM/PLACEBO CONTROLLED RHTN TRIALS Control Arm Changes from Baseline Met EP EP Not Met Met EP EP Not Met EP Not Met N=132 BL to 14 wks N=120 BL to 14 wks N=56 to 8 weeks . N=84 0 to 6 mo. N=171/159 to 6 mo.
Pre-Specified Subgroup Analysis mm Hg RDN Better Control Better * ITT population, 5 mm Hg superiority margin test .
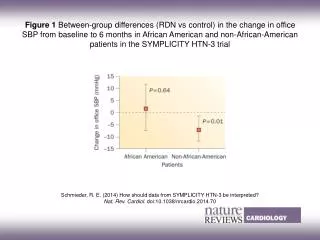
Demographics and Control Group Impact RDN AA N = 85 N-AA N = 264 mm Hg Control AA N = 49 N-AA N = 120 mm Hg Vasodilators are dosed up to 4x daily, making compliance a challenge
Aldosterone Antagonists Sub Group Aldosterone Antagonist Subgroup Efficacy AA at Baseline AA at Baseline No AA at Baseline No AA at Baseline N=274 N=76 N=47 N=73 N=122 N=113 N=252 N=46 P = 0.574 mm Hg mm Hg RDN P = 0.219 P = 0.127 Control P = 0.098 Office BP Ambulatory BP
HTN-3: Procedural Experience 5X more operators vs HTN-1 Greater heterogeneity of operator experience vs. HTN-1 and HTN-2 Case proctoring was different and not comparable
HTN-3: Continuing Areas of Investigation Heterogeneity of US Operator Experience Patient Demographics Catheter Design Medication Changes or Adherence ? ? Trial Conduct Hawthorne Effect Placebo Effect Regression to Mean
Medtronic Next Steps • Medtronic will continue to provide access to the Symplicity™ system in countries where it has regulatory approval and will continue to support a global hypertension clinical program. • Medtronic will continue to enroll in the Global SYMPLICITY Registry. • Our detailed analyses of HTN-3 suggest that further investigation is warranted; Medtronic is in discussions with the FDA to determine the path forward for the next US IDE trial. • In light of the results of the SYMPLICITY HTN-3 trial, Medtronic will discontinue the already suspended SYMPLICITY HTN-4 trial • Medtronic will consult with local regulatory bodies to determine the future of the HTN-Japan and HTN-India clinical studies. • Medtronic will continue to pursue its studies in other disease states, including AF, CKD, HF, etc.
Key Takeaways • SYMPLICITY HTN-3 did not reach the primary or powered secondary efficacy endpoints in this trial. There may be many factors that contributed to the outcome, which we continue to investigate. • SYMPLICITY HTN-3 did meet its safety endpoint, which is consistent with all other Symplicity trials, including the Global SYMPLICITY Registry. • Based upon our detailed analysis of HTN-3, we believe further clinical investigation is warranted and Medtronic will, in consultation with FDA, pursue a new IDE trial • An unmet need in this uncontrolled hypertension population still exists. Medtronic will continue to provide access to the Symplicity system in countries where it has regulatory approval and will continue to support a global hypertension clinical program
www.medtronic.com www.medtronicRDN.com United States Medtronic USA, Inc. 3576 Unocal Place Santa Rosa, CA 95403 USA Tel: 707.525.0111 LifeLine Customer Support Tel: 877.526.7890 Tel: 763.526.7890 Product Services Tel: 888.283.7868 Fax: 800.838.3103 Europe Medtronic Intl. Trading SARL Route du Molliau 31 Case Postale CH-1131 Tolochenaz Switzerland Tel: 41.21.802.7000 Fax: 41.21.802.7900 Canada Medtronic of Canada Ltd. 99 Hereford Street Brampton, Ontario L6Y0R3 Canada Tel: 905.460.3800 Fax: 905.460.3998 Toll-free: 800.268.5346 Asia Pacific Medtronic Intl. Ltd. 49 Changi South Avenue 2 Nasco Tech Center Singapore 486056 Singapore Tel: 65.6436.5000 Fax: 65.6776.6335 Latin America Medtronic USA, Inc. Doral Corporate Center II 3750 NW 87th Avenue, Suite 700 Miami, FL 33178 USA Tel: 305.500.9328 Fax: 786.709.4244
Results: Blinding Efficacy *The lower boundaries of the confidence intervals of the blinding index are both >0.5, indicating sufficient evidence for blinding.
Sample Size Assumptions • SYMPLICITY HTN-3 sample size was driven by the safety endpoint, a composite of Major Adverse Events (MAE). • Safety endpoint compared to an Objective Performance Criterion (OPC) of 9.8%, derived from historical data. • 316 RDN therapy group subjects were required to provide 80% power, using a one-sided significance level of 0.05. • Given 2:1 randomization, 158 control group subjects were required. • Accounting for expected patient attrition, sample size was increased to a minimum of 530 randomized total patients • MAE was defined as all-cause mortality, ESRD, embolic event resulting in end-organ damage, renal artery or other vascular complication, hypertensive crisis through 30 days, including new renal artery stenosis within 6 months.
HTN-3: Different Control Response in African American Population
SYMPLICITY HTN-1: Significant, Sustained BP Reduction to 3 Years 6 Months (N = 144) 1 Year (N = 132) 2 Years (N = 105) 3 Years (N = 88) Change in Blood Pressure (mm Hg) Systolic Diastolic P < 0.01 for from baseline for all time points. Data is reported only on the patients available at each time point. Expanded results presented at the European Society of Cardiology Annual Meeting, 2013.
SYMPLICITY HTN-2: BP Reductions Sustained to 3 Years Sustained Reductions in the Pooled (RDN and Crossover) Group* 6 Months N = 84 12 Months N = 80 18 Months N = 74 24 Months N = 69 30 Months N = 69 36 Months N = 40 ∆ From Baseline to 36 Months (mm Hg) Systolic Diastolic P <0.01 at all time points *Crossover patients only had 30 months post-procedure data. Whitbourn, TCT 2013
Multiple Unblinded Trials Show RDN Lowers Blood Pressure N=313 N=102 N=346 N=153 N=63 N=146 N=15 N=109 N=46 N=15 Medtronic N=47 EnligHTN/St Jude Vessix/Boston Sci. Maya/Covidien Recor Published Sources: Lancet 2009 Lancet 2010 TCT 2013 Journal of Human Hypertension 2013 Circulation 2013 Clin Res Cardiol2013 J Am SocNephrol2012 Eur Heart J 2013 TCT 2013 Eurointervention 2013 EuroIntervention 2013 Mean Decrease in Office Systolic Blood Pressure at 6 Mo (mm Hg)