Download
1 / 15
200 likes | 443 Vues
Medical Management of Ulcerative Colitis. Alistair Makin Manchester Royal Infirmary. Treatment Choice. Dependent on Acute attack or maintenance of remission Assessment of Disease Severity (Truelove & Witts 1950’s) Mild - < 4 stools /day, no systemic disturbance, normal ESR

E N D
Medical Management of Ulcerative Colitis Alistair Makin Manchester Royal Infirmary
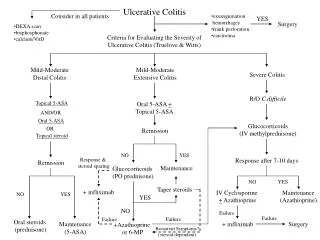
Treatment Choice Dependent on • Acute attack or maintenance of remission • Assessment of Disease Severity (Truelove & Witts 1950’s) • Mild - < 4 stools /day, no systemic disturbance, normal ESR • Moderate - > 4 stools/day but with minimal systemic upset • Severe - > 6 stools/day with blood, evidence of systemic disturbance – fever, tachycardia, anaemia or ESR >30 • Toxic dilatation • Extent of disease (topical v systemic)
The Acute Attack Mild to Moderate Disease Salicylates • Sulfasalazine (SASP) first used in 1942 • Response rate of 60% • 25-30% adverse effects • Newer 5-ASA fewer side effects ( 10%) • Topical + systemic dosing more effective • Cochrane Review 4/1/03 • Newer 5-ASA preparations superior to placebo and trend to benefit over SASP. Considering relative costs a clinical advantage of newer 5-ASA v SASP is unlikely
New 5-ASA Preparations • Balsalazide (azo-bonded prodrug) v mesalamine • 46% v 44% achieved remission • Response rate 68% v 61% in new diagnosis • 36% v 25% in relapse • Symptomatic remission 25 v 37 days Pruitt et al 2002 • Balsalazide v sulfasalazine • Similar response rate • Patient withdrawal 7% v 31% Green et al 2002
The Acute Attack Role of Steroids • First used in 1950’s • Severe attack mortality reduced from 37% to < 1% • Topical for left-sided disease • Oral for more extensive disease or failed local Rx • 40mg/d more effective than 20mg/d • 60mg/d > 40mg/d but more side effects Baron et 1962 • IV initially in severe disease
The Acute Attack – when Steroids Fail Predictors of failed medical therapy Failure Rate • > 8 stools/day 33% • Pulse > 100 36% • Albumin < 30g/l 42% • Temp > 38°C 56% • Mucosal islands on plain AXR 75% • Small bowel dilatation 73% • Colonic dilatation 75% Lennard-Jones 1975 Chew et al 1991 • Surgery - failure to respond after 5 days
Salvage Therapy Cyclosporin • Oxford data • Initial pilot suggested benefit • Dual centre controlled trial of patients failing to respond at day 5 • IV cyclosporin (4mg/kg) + steroids v conventional Rx • 9/11 on cyclosporin responded v nil • 60% still well at 6 months • New York Data • Similar benefit • 54/111 patients major toxicity (2 deaths, 7 severe infections)
Cyclosporin • St Marks Data – low dose 2mg/kg • 31 patients • 11 cyclosporin + steroids 2(18%) urgent - 5(25%) delayed colectomy • 20 cyclosporin 5(25%) urgent – 5(25%) delayed colectomy • Benefit with concurrent azathioprine
Salvage Therapy Azathioprine Slow onset of action Loading IV onset of action still 4 weeks Methotrexate No role Infliximab Anecdotal evidence but no convincing trial data
Cuckoo Land ? • Antibiotics No established role • Probiotics – commensal bacterial species Possible role of VSL#3 (a combination of 4 lactobacillus species) in mild-moderate disease • Trichuris suis eggs • (Porcine Whipworm) • 86% remission • 85% relapse by 12 weeks • Remission maintained with 3/52 repeat doses
Remission • No role for steroids • Sulfasalazine – reduced relapse rate 4-fold • Newer 5-ASA’s comparable • What Dose? • How long for? Long-term at appropriate dose for preparation used
Novel Approaches • Oral 5-ASA + twice weekly enemas v oral alone Reduction in number and incidence of relapses Higher chance of no relapse More costly but decreased relapse & hospital costs Piodi et al 2004 • Patient-led variable dosing Balsalazide 1.5g bd with 750mg increments up to 6g for 7 days if symptoms increased • Stable remission – 44% relapse by 3 years • Newly in remission - 59% Green et al 2004
Azathioprine Converted to 6-MP in liver and then to thioinosinic acid which impairs purine biosynthesis - inhibits cellular proliferation - slow onset of action as act on newly differentiating cells • Induction & maintenance of remission in refractory disease • 66% response rate • Need 3 months of treatment to determine response • 10% intolerant • Myelosuppression 5% in first 6 months • Late complications so prolonged monitoring needed
Azathioprine • Dose 2mg/kg • 3 monthly FBC/LFT’s once stable • Stop if WBC <3•5 or neutrophils <1•5 • How long for? • Relapse rates on AZA 11%-1 year 32%-5years • Relapse rates higher if AZA stopped than if continued up to year 4 of treatment • when AZA stopped when in remission but >6months Rx 38%-1 year 75%-5 years • No increase in relapse rates when Rx > 5 years • Treat for a minimum of 4 years
Conclusions • Determine severity of attack and treat appropriately • Topical v systemic • Limit steroid use (DEXA scan if > 3months of 7.5mg.d) • Consider immunosuppression early • Duration of treatment important • Joint management with surgeons of severe and refractory cases • The worms are coming!