Download
1 / 15
200 likes | 837 Vues
ULCERATIVE COLITIS. Presentation :Dr.Doaa AL-Masri. Attendance :Dr.Yousef Abu-Osbaa. Discussion :Dr.Hisham Al-Nazer. History . Mohammad is 5 years old male patient, who was referred from the West Bank as a case of ulcerative colitis for further evaluation. . History.

E N D
ULCERATIVE COLITIS Presentation :Dr.Doaa AL-Masri. Attendance :Dr.Yousef Abu-Osbaa. Discussion :Dr.Hisham Al-Nazer.
History • Mohammad is 5 years old male patient, who was referred from the West Bank as a case of ulcerative colitis for further evaluation.
History • At 4 months of age, he had large amount of watery diarrhea 4-6 times/day mixed with mucous and blood, with occasional vomiting. • He was managed as cow’s milk protein allergy without improvement for the next 5 months.
History • At 9 months of age, ulcerative colitis was diagnosed by colonoscopy. • Treated with Prednisone, Sulfasalazine and Multivitamins, with no improvement. • Diarrhea continued with exacerbation by infections, associated with poor weight gain and loss of appetite. • He was referred to Jordan Hospital for further evaluation.
History • Vaccination up to age. • Nutritional history: • Breast fed till the age of 2 years. • Semisolid food was introduced at the age of 6 months . • Now he eats regular food but with poor appetite.
History • Development history: appropriate for age. • Family history : unremarkable. • Social history: unremarkable.
Physical examination • The patient looked ill, pale,wasted, not jaundiced. • Normal vital signs. • Weight : 12.5 kg ( 3 standard deviation below the mean) . • Length : 92cm ( 4 standard deviation below the mean).
Physical examination • Head & Neck : No oral ulcers. • Chest: Good air entry bilaterally. No added sounds. • Heart: Normal S1, S2. No murmur . • Abdomen : soft, and lax. No tenderness. No palpable organs. • Normal male genitalia. • Anal orifice : normal. • CNS: Grossly intact. • Lower limbs: Muscle wasting.
Investigations • Hb. : 9.4 gm/dl • PCV : 30.4 gm/dl. • MCV: 61fl- MCH : 19 pg –MCHC:30.9 g/dl • WBC: 23.9/L: • - Neutrophil : 40%.- Lymphocyte:44% • -Monocyte : 4%. - Eosinophil : 2%. • Blood film : Neutrophils showed left shift
Investigations • Liver function test :normal. • Kidney function test: normal. • Urinanalysis and culture: negative. • ESR : 90 mm/1st hour. • CRP : 48mg/l. (Normal <6 mg/dl ). • Wrist X-ray: delayed bone age ( 2.5 y).
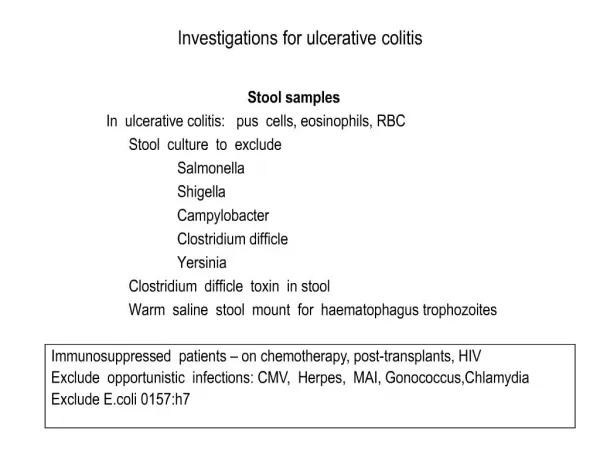
Investigations • Stool Rotazyme: negative. Culture : no growth, occult blood: positive , colour : green, appearance : soft, WBC ; 42/HPF, RBC : 55/HPF , E. histolytica cyst and trophozoite. • Stool analysis was repeated after 7 days of Metronidazole and it was negative for ova and cyst but many budding yeast were seen.
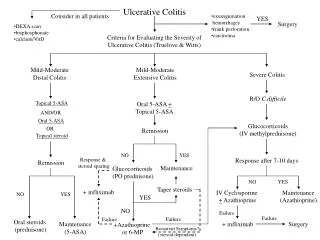
Course in hospital The patient was started on: • Metronidazole. • Mesalazine . • Prednisone . • Azathioprine.
Course in hospital • The patient developed severe diarrhea with poor oral intake and severe dehydration, hyponatremia and hypokalemia resulted and so I.V fluids were started for rehydration. -Oral thrush and budding yeast in stool so, Nystatin and Mycoheal was given.
Medication on Discharge Azathioprine 12.5 mg P.O Q 12 hr. Prednisone 5 mg tab Q 6 hrs. Mesalazine 250mg Q12hr.