Download
1 / 60
660 likes | 875 Vues
Orthotic Treatment of The Neuropathic Diabetic Foot. David Kingston BSc. (Hons) MBAPO SR P/O Senior Orthotist IDS Cappagh Hospital. Orthotist. Four year B.Sc.(Hons) Dual qualified BAPO State Registered. Training. Introduction.

E N D
Orthotic Treatment of The Neuropathic Diabetic Foot David Kingston BSc. (Hons) MBAPO SR P/O Senior Orthotist IDS Cappagh Hospital
Orthotist • Four year B.Sc.(Hons) • Dual qualified • BAPO • State Registered
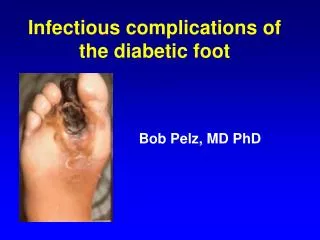
Introduction • Foot complications are one of the most serious and costly complications of NIDDM. • Amputation of (or part of) a lower limb is usually preceded by a foot ulcer • A strategy which includes prevention, patient and staff education, multi-disciplinary treatment of foot ulcers and close monitoring can reduce amputation rates by 49-85% • In May 1999 the WHO and International Diabetes Federation set goals to reduce the rate of amputations by 50% in five years • They (We) have failed
Pathophysiology • Spectrum of foot lesions varies across the world • Pathways are almost identical • Up to 50% of NIDDM patients have neuropathy and at-risk feet • Neuropathy leads to an insensitive and subsequently deformed foot with possibly an abnormal gait • Trauma can lead to a chronic ulcer • Loss of sensation, foot deformities and limited joint mobility can lead to abnormal biomechanical loading of the foot
As a normal response to pressure a callous is formed • The skin finally breaks down • Frequently preceded by a subcutaneous haemorrhage • The patient continues to walk on the insensate foot impairing healing • Lack of treatment can lead to the need for amputation • Once a patient has an ulcer they are 77 times more likely to get a second ulcer after treatment of the first has healed the ulcer • Once amputation has occurred then the pressures on the remaining limb increase
Five Cornerstones of the Management of the Diabetic Foot • Regular inspection and examination of the foot at risk • Identification of the foot at risk • Education of patient, family and healthcare providers • Appropriate footwear • Treatment of non-ulcerative pathology
Rearfoot Valgus Rearfoot Varus Forefoot Valgus Forefoot Varus Hallux Valgus Hallux Limitus Hallux Rigidus FHL Claw Toes Hammer Toes Mallet Toes First Ray Dysfunction Prom Met Heads Morton’s Syndrome Tailors Bunion Forefoot Ab/Adductus Foot Deformities
Sensory loss due to diabetic polyneuropathy can be assessed using the following techniques
Treatment of non-ulcerative pathology • Skin care • Regular Chiropody • Nail care • Diabetic Footwear • Diabetic Socks • Diabetic Insoles • Oedema control
Orthotic Treatment - Low Risk • Education • Socks • Footwear – Stock • Insoles
Patient Education • Take care of your diabetes control • Check your feet daily • Wash your feet daily • Keep your skin soft and smooth • Smooth corns and calluses gently • Trim your toenails regularly and carefully • Wear socks and shoes at all times • Protect your feet from heat and cold • Keep the blood flowing to your feet • Be more active • Consult your GP
Appropriate Footwear • Good leather • Lace up • Solid one piece sole • Padded collars • Soft toe puff • Good lining • No stitching or intricate designs • Low heels • No tapered heels • Regular soling • Good fit
Footwear Objectives • Relieve areas of plantar pressures • Reduce shock • Reduce shear • Accommodate deformities • Stabilize and support deformities • Limit motion of joints
Orthotic Treatment - Medium Risk • Education • Socks • Footwear – Stock or Bespoke • Insoles
Orthotic Treatment - High Risk • Education • Socks • Footwear – Stock or Bespoke • Insoles
Treatment of Ulcers • Relief of pressures • Restoration of skin perfusion • Treatment of infection • Metabolic control (<10 mmol) • Local wound care • Instruction of patient and relatives • Determination of the cause and preventing recurrence
Orthotic Treatment - Ulceration • Footwear – Bespoke • Insoles • PRAFO • CROW Walker • Total Contact Cast • Pneumatic Walker • Rest
Neuropathic Ulcers • Sensory Loss • Trauma • Callous • Ulceration
Charcot Foot • Neuro-arthropathy that affects the joints in the foot • Rapidly progressive degenerative arthritis that results from neuropathy • Pain perception and the ability to sense the position of the joints in the foot are severely impaired or lost • Muscles lose their ability to support the joint(s) properly. • Loss of these motor and sensory nerve functions allow minor traumas such as sprains and stress fractures to go undetected and untreated • Leads to ligament laxity, joint dislocation, bone erosion, cartilage damage, and deformity of the foot • Joint effusions, large osteophytes, fractures, bone fragments, and joint misalignment and/or dislocation
Charcot Foot – Six Key Points • The acute Charcot foot can mimic cellulitis or, less commonly, deep venous thrombosis • The existence of little or no pain can often mislead the patient and the physician • Findings on plain x-rays can be normal in the acute phase of the Charcot foot • Strict immobilization and protection of the foot is the recommended approach to managing the acute Charcot process • A careful program of patient education, protective footwear and routine foot care is required to prevent complications such as foot ulceration • Reconstructive surgery is reserved for patients who have recurrent ulceration despite compliance with the previously mentioned regimen