Download
1 / 10

E N D
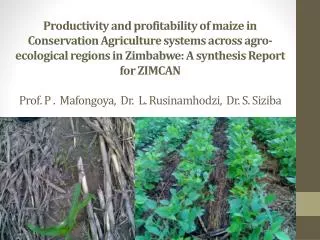
Special IARIW-SAIM Conference on “Measuring the Informal Economy in Developing Countries”, Kathmandu, Nepal, September 24-26,2009 NGOs and NPISHs in Health Sector: Possibilities and Policy Options; An Exploratory Study in the Indian ContextP.M. MathewChrist UniversityBangalore, IndiaDiscussant M.R. Narayana, Ph.DProfessor of EconomicsInstitute for Social and Economic ChangeBangalore, India
FOCUS AND METHODOLOGY OF THE PAPER FOCUS • Description of the role of NGOs (specially, voluntary organizations) in delivery of health services in India with special reference to their health expenditure • Brief review of literature on NGOs in health sector • Distinction of types of NGOs • Select problems of NGOs • Policy options, supported by case studies METHODOLOGY • Descriptive and positive analysis • Based on secondary data • Case studies
Role and advantages of NGOs • Supplementary to existing service providers with focus on vulnerable sections of society (e.g. poor, slum dwellers and tribal populations) in rural areas (mainly village based)- useful to fill in health gaps • Low cost delivery of services, due to less expenditure on salaries and wages, and voluntary services by people • Close to people with more opportunities for identifying disadvantaged people and their health needs • Open for diversified participation: charitable institutions, religious organizations, internal and external individuals and institutions through donations and collaborations • Flexibility in operations – combining health care delivery with income generation programmes – Integrated development programmes
Size of health care NGOs and their services: Select estimates Independent Commission of Health in India 1997: Number of NGOs =7000 Directory of Hospitals 1998 – 10 percent of all hospitals (937) and 13 percent of all beds (74498) in non-profit sector Background paper for National Commission on Macroeconomics and Health 2005 - Christian missionary hospitals leads the provisioning of health services – 47 percent of all beds in private sector and 17 percent of all private hospitals/dispensaries
Health care expenditure by NGOs:Select estimates National Health Accounts India (NHAI) 2001-02: 0.1 percent of total expenditure (Household expenditure=72 percent) National Commission of Macroeconomics and Health 2005: 0.3 percent of total expenditure (Household expenditure=70 percent) Major items of expenditure: Curative medicine & recurring - About 98 percent Major sources of financing – NHAI 2001-02 Grants from government=26.7 percent; User charges in hospitals and dispensaries=38.9 percent; and external assistance=25.5 percent
Problems of health care NGOs • Insufficient resources- non-remuneration for health staff and workers and inadequate training; high turnover of middle-level staff; dependency on donor agencies • Inefficient management including commercial operations (e.g. charging higher user fees) to meet with insufficient resources • Superficial forms of local participation • Lack of community ownership • Lack of policy directions – non-announcement of National Policy on Voluntary Sector
Policy options (specially for additional resource mobilization and subsidization) • Community Health Insurance (CHI) – Ashwini in Niligiri Hills in Tamil Nadu state since 1992 – CHI for tribal population covering 13000 members – insurance reimbursements contributed around 50 percent of total hospital income in 2006-07 • Boutique Healthcare – an instrument of cross-subsidization – L.V. Prasad Eye Institute in Hyderabad (LVPEI)– 50 percent of patients are treated free of cost – Aravind Eye Hospital in Madurai – 70 percent are treated free of cost • Healthcare-Microfinance Linkages – National Dawakhana in Nanded city empowers women and improves their ability to pay for health services
Policy options (specially for additional resource mobilization and subsidization) • Donor Marketing and Product sales – LVPEI • Private-public partnerships – co-operative sharing of health facilities (West Bengal government in 2004) – management of PHC by Sewa Rural at Jhagandia block in Baruch district for ten years from 1989 to 1999- MNGO/FNGO/SNGO programme for RCH services in Orissa • International collaborations – Project ORCHID in Manipur in collaboration with Australian International Health Association and Emmanuel Hospital Association-Ankur Project-SEARCH in Maharashtra in collaboration with Save the Children USA and Bill and Melinda Gates Foundation • Consultancy Services – through creations of Centres of Excellence
Discussion points • Relative efficiency between NGOs and other providers of health care services • Role of health care NGOs in Indian System of Medicine • Distinction between NGOs, voluntary organizations and NPISHs, and their relationship with informal sector • Corporate social responsibility through foundations and NGOs • Beneficiaries of health care NGOs and informal workers and their dependents • Lessons from experiences in other developing countries