Download
1 / 9
100 likes | 269 Vues
Benign prostateic hyperplasia. Dept. of urology.Shanghai Renji hospital Wang YiXin. Etiology of BPH . The etiology of BPH IS undoubtedly multifactorial. However,it is well recognized that two prerequisites for its induction are the testes and aging .

E N D
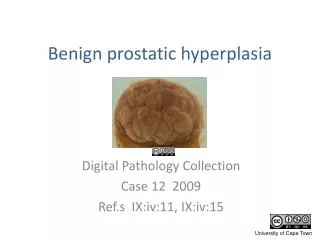
Benign prostateic hyperplasia Dept. of urology.Shanghai Renji hospital Wang YiXin
Etiology of BPH • The etiology of BPH IS undoubtedly multifactorial. However,it is well recognized that two prerequisites for its induction are the testes and aging . • Because prostatic growth is regulated principally by androgen. • It has been suspected for years that BPH is under endocrine control .In addition. There is compelling evidence for a major role of the stroma in the induction of the disease .
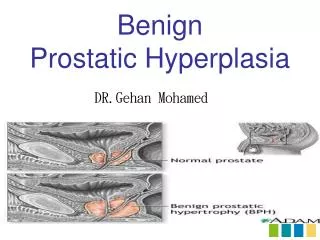
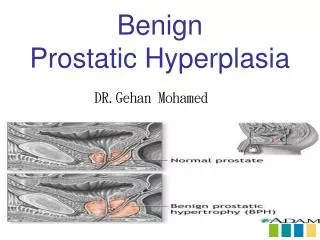
Pathology of BPH • The basic change is that of epithelial hyperplasia of the prostatic glands and their fibrous stroma • A wide variation between epithelial and fibrous elements. • The hypertrophy originates in the periurethral glands • Form a false capsule.
Local symptoms Increased frequency Nocturia ,hesitancy Feeling of incomplete Emptying . Dribbling, Dysuria. Haematuria, Epididymitis Urgency, Incontinence. Micturition easier on squatting General symptoms Lassitude due to nocturia. Renal pain. Prinephric abscess . Progressive renal failure. Anorexia ,Nausea, Vomiting Dyspnoea,Coma. Clinical features
Diagnosis of BPH • Clinical history • General examination • Rectal examination :size,consistency, irregularities or hard nodules. • Becteriological tests:MSU (meadum stream urine) • Haematological tests:anaemia • Biochemical tests:blood urea and creatinine, electrolytes, PSA.
Diagnosis of BPH(Radiology) • Straight x-ray, KUB. • IVP shows: 1.suppression of renal function 2.hydronephrosis and hydroureter 3.fish-hooking of the lows ends of the ureter 4.trabeculation of the bladder 5.bladder diverticular formation 6.filling defects in the bladder 7.residual contrast left in the bladder after micturition • RGP,when non-functioning kidney is present.
Other investigations • Electro—cardiography to assese myocardial state • Chest x—ray • Pulmonary function tests
Treatment of BPH • Chronic retention of urine • Acute retention • Conservative methods by running water taps to induce to void ,sitting in a warm bath • Catheterrisation • Suprapubic cystostomy:temporary form of suprapubic cystostomy,catheter should be changed at monthly.
Operative treatment of BPH • Transurethral prostatectomy • Retropubic prostatectomy • Transvesical prostatectomy • Transperineal prostatectomy • Cryogenic prostatectomy • Microwave therapy