Download
1 / 44
560 likes | 851 Vues
Porphyrins & Bile Pigments. Objectives. After studying this chapter, you should be able to: Know the relationship between porphyrins and heme Be familiar with how heme is synthesized Understand the causes and general clinical pictures of the various porphyrias

E N D
Objectives • After studying this chapter, you should be able to: • Know the relationship between porphyrins and heme • Be familiar with how heme is synthesized • Understand the causes and general clinical pictures of the various porphyrias • Know how bilirubin is derived from heme and how it is handled in the body • Understand the nature of jaundice and appreciate how to approach determining its cause in a patient.
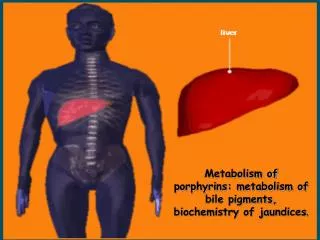
Hemoproteins • Heme • Porphyrias (Inherited) • Catabolism of the heme • Jaundice (causes of)
The porphyrins • The porphin nucleus • Methenyl bridges • Pyrrole ring • Side chains
Arrangement of the substituents • Side chains • Asymmetric substitution • Type III porphyrin • More abundant • Symmetric arrangement • Type I porphyrin
ALA Synthase Is the Key Regulatory Enzyme in Hepatic Biosynthesis of Heme • ALAS1 • ALAS2 • Heme • Repression-derepression mechanism • Translation of the enzyme • Its transfer from the cytosol to the mitochondrion • Drugs • Cytochrome P450 • Utilization of heme
Glucose • Hematin • (ALAS2) • Not induced by the drugs • Does not undergo feedback regulation by heme
The porphyrias • 85% of heme synthesis occurs in erythroid precursor cells in the bone marrow and the majority of the remainder in hepatocytes • Erythropoietic or • Hepatic
THE PORPHYRIAS ARE GENETICDISORDERS OF HEME METABOLISM • Genetic or acquired • Diagnosis • Assay of the activity • eg, red blood cells • Use of appropriate gene probes • Prenatal diagnosis
The Porphyrias are GeneticDisorders of Heme Metabolism • The signs and symptoms of porphyria result from • Deficiency of metabolic products • Deficiency of heme • Accumulation of metabolites behind the block • Prior to the formation of porphyrinogens • ALA and PBG will accumulate • Abdominal pain and neuropsychiatric symptoms • Later in the pathway • Accumulation of the porphyrinogens
Porphyrias • Treatment • Avoid drugs that cause induction of cytochrome P450 • Repress ALAS1 • Glucose loading • Hematin • β-carotene • Lessen production of free radicals • Sunscreens
Catabolism of heme produces bilirubin • Hemoglobin • Globin • Iron • Porphyrin • Hemoglobin • Ineffective erythropoiesis • other heme proteins • Cytochrome P450 • Reticuloendothelial cells
Hyperbilirubinemia • Bilirubin in the blood exceeds 1 mg/dL • Overproduction • Failure of a damaged liver to excrete bilirubin • Jaundice or icterus • 2–2.5 mg/dL • Direct reacting • React without the addition of methanol • Indirect-reacting
Kernicterus • Unconjugated bilirubin can cross the blood-brain barrier
Elevated UnconjugatedBilirubin in Blood • HEMOLYTIC ANEMIAS • Usually only slight (< 4 mg/dL) • NEONATAL “PHYSIOLOGIC JAUNDICE” • Accelerated hemolysis • Immature hepatic system • CRIGLER-NAJJAR SYNDROME • TYPE I • Serum bilirubin usually exceeds 20 mg/dL • Mutations in the gene encoding bilirubin-UGT
Elevated UnconjugatedBilirubin in Blood • TYPE II • Some activity of the enzyme is retained • Usually do not exceed 20 mg/dL • GILBERT SYNDROME • Mutations in the gene encoding bilirubin-UGT • 30% of the enzyme’s activity is preserved • Harmless
Elevated UnconjugatedBilirubin in Blood • TOXIC HYPERBILIRUBINEMIA • Acquired disorders • Liver dysfunction • Impairs conjugation
Conjugated Hyperbilirubinemia • OBSTRUCTION OF THE BILIARY TREE • DUBIN-JOHNSON SYNDROME • ROTOR SYNDROME
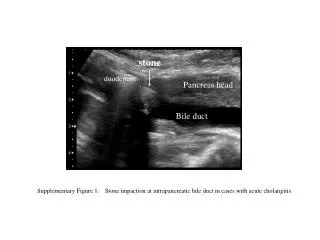
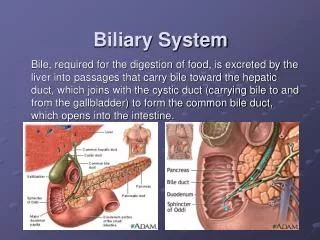
OBSTRUCTION OF THE BILIARY TREE • Due to • Gallstone • Cancer of the head of the pancreas • Cholestatic jaundice • Include • All cases of extrahepatic obstructive jaundice • Micro-obstruction of intrahepatic biliary ductules
DUBIN-JOHNSON SYNDROME • Benign autosomal recessive • Mutations in the gene encoding MRP-2 • Secretion of conjugated bilirubin into bile
ROTOR SYNDROME • Rare • Benign • A chronic conjugated hyperbilirubinemia • Normal liver histology
Delta bilirubin • Longer half-life
Laboratory results in normal patients and patients with three different causes of jaundice. • Hepatitis • Damage to parenchymal cells • Micro-obstruction to bile ductules
Causes of jaundice • Prehepatic • Hepatic • Posthepatic • Distinction • Measurement of prothrombin time • Electrophoresis of proteins • Activities of the enzymes ALT,AST, and alkaline phosphatase
Causes of jaundice • Measurements of plasma • Total and Nonconjugated bilirubin • Urinary • Urobilinogen and bilirubin