Download
1 / 62
620 likes | 753 Vues
Concept 14: HIV/AIDS. Fall 2011 Barbara E. Connell, RN, MSN. Overview. 1981 5 cases of PCP and 26 cases of Kaposi’s Sarcoma diagnosed in young, healthy gay men LA and NY Labeled Acquired Immunodeficiency syndrome 1984 the HIV (retrovirus) isolated Was spread primarily by sexual contact .

E N D
Concept 14: HIV/AIDS Fall 2011 Barbara E. Connell, RN, MSN
Overview • 1981 • 5 cases of PCP and 26 cases of Kaposi’s Sarcoma diagnosed in young, healthy gay men • LA and NY • Labeled Acquired Immunodeficiency syndrome • 1984 the HIV (retrovirus) isolated • Was spread primarily by sexual contact
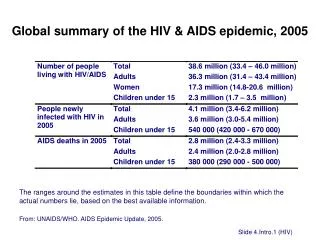
Overview cont. • Became apparent that AIDS was the final, fatal stage of HIV infection • Is now a world wide concern • Estimated 36.2 million infected • Highest incidence in sub-Sarahan Africa (70%) • No vaccine or cure • Progression of disease has been slowed due to HAART: highly affective antiretroviral therapy
Pathophysiology and Etiology • AIDS is caused by the HIV • Best example of primary immunodeficiency disorder • Present in blood, semen, vaginal and cervical secretions, and cerebrospinal fluid • Also found in breast milk and saliva • Sexual contact primary mode of transmission • Transmitted through blood, needle sharing
Pathophysiology and Etiology cont. • Approx 13-40% of infants born to infected mothers are infected perinatally • The virus infects cells that have the CD4 antigen • Once inside the cell, the virus sheds its protein coat and uses reverse transcriptase to convert the viral RNA to DNA • The viral DNA is then integrated into host cell DNA, and duplicates during cell division
Pathophysiology and Etiology cont. • Virus may remain latent • May become activated to produce new RNA and form virions (produce outside a host) • It then buds from the cell surface, disrupts the cell membrane, destroys host cell • With inactive virus: antibodies are produced • This is called seroconversion • Antibodies detected about 6 wks/6months
Pathophysiology and Etiology cont. • Helper T and CD4 cells are primary ones infected • Also infects macrophages and certain cells in the CNS • Helper T cells: recognize foreign antigens and infected cells • Also activate antibody producing B cells • Direct cell-mediated immune activity
Pathophysiology and Etiology cont. • Also direct cell-mediated immune activity • Influence the phagocytic activity of monocytes and macrophages • Loss of helper T cells leads to immunodeficiencies • Children: perinatal transmission (vertical transmission), transmission during birth (blood or genital tract secretions), breast milk
Pathophysiology and Etiology cont. • Risk reduced when mothers identified receive zidovudine (Retrovir, AZT) during pregnancy, deliveries by c-section, therapy after birth • Mandatory blood screening instituted in 1985 • Prior to 1985 children infected during treatment of hemophilia • Today: infected through unprotected sex
Etiology • 1981-2006: 982,498 cases U.S. • 2006: 35,314 new cases in the 33 states with long-term reporting data • Men: majority of cases, women only 26% • Females: high-risk heterosexual contact (80%), drug use (19%), other (1%) • African-American and Latino (82%) • 2001-2004: 15, 338 children and teens
Etiology cont. • The most rapid increases have been seen in young gay and bisexual men, women, inner-city drug users • Rate of perinatal transmission has declined dramatically • Death from AIDS has decreased due to improved treatment modalities • Increase in older persons contracting the disease
Risk Factors • Behavioral • Men • Gays, bisexuals, prison population • Unprotected anal intercourse • Injection drug use • Women • Heterosexual intercourse with infected drug user • Trading sex for drugs
Risk Factors cont. • Hemophilia and blood transfusions • Screening for high-risk behavior has reduced the number of donors found to be positive • Risk of contracting disease from blood donors limited to those who may be in the window period (have no detectable antibodies yet) • Health care as an occupation • Needlesticks or nonintact skin with exposure to an infected individuals body fluids
Risk Factors cont. • Poverty • Increases one’s risk for HIV/AIDS • Have less access to preventive health care and health care education • Risk for increased illiteracy • Less likely to have access to internet • African American women greater risk
Risk Factors cont. • Pregnancy and breast feeding • Perinatal transmission risk factors: cigarette smoking, illicit drug use, genital tract infections, unprotected sexual intercourse: multiple partners • Infants usually positive after birth, does not mean they are infected • Avoid breast feeding if possible
Risk Factors cont. • Older adults • Fail to use condoms, because they are past child bearing age • Believe they cannot contract the disease • May have delayed diagnosis and increased severity of the disease • Need routine screening for anyone who has risk factors
Risk Factors cont. • Myths and misconceptions • Not transmitted by casual contact • Nor by mosquitoes • Only by contact with blood and body fluids • Newer drugs are improving the longevity of infected people • Early detection improves outcomes • May be difficult to dispel peoples beliefs • Many believe if not homosexual or IV drug users they don’t need to worry
Clinical Manifestations • Often contribute initial manifestations to a common viral illness • Following the acute illness, clients enter a long-lasting asymptomatic period • Virus is present and can be transmitted to others • Asymptomatic period varies: mean duration is 8-10 years • May develop generalized lymphadenopathy
Clinical Manifestations cont. • Diarrhea • Oral lesions, hairy leukoplakia, candidiasis, and gingival inflammation and ulceration • Advanced HIV typically occurs 10-11 years after initial infection • Varies according to viral load, rate of disease progression, development of resistance to antiretroviral therapy
Clinical Manifestations cont. • AIDS • Neurologic manifestations • Opportunistic infections • Cancers • Categorized by clinical symptoms and by T4 cell counts • Antiretroviral therapies stop or suppress the activity of a retrovirus
Clinical Manifestations cont. • They prevent further weakening of the immune system • Minimize opportunistic infections • AIDS: survival 2-3 years after diagnosed • PCP infection • In undiagnosed individuals • Have a late diagnosis of HIV infection • Fail to take prophylactic antibiotics when CD4 count is less than 200/mm3
AIDS Dementia Complex • Neurologic manifestations: affect 40-60% of those with AIDS • Include dementia, delirium, seizures • From virus and opportunistic infections • Impacts cognitive, motor and behavioral functioning • Fluctuating memory loss, confusion, difficulty concentrating, lethargy, diminished motor speed
AIDS Dementia Complex cont. • Become apathetic • Leads to severe dementia • Ataxia, tremor, spasticity, incontinence, paraplegia • Toxoplasmosis and non-Hodgekin’s lymphoma • May cause H/A, altered mental status, neurologic deficits • Develop neuropathies: numbness, tingling, pain in LE’s • May develop inflammatory demyelinatingpolyneuropathy • This is similar to Guillain-Barre
Opportunistic Infections of AIDS • Normal CD4 counts: greater than 1,000/mm3 • Immunodeficiency develops below 500/mm3 • CD4 less than 200/mm3: opportunistic infections and cancer are likely • PCP: most common, about 80% develop it at some time during their disease • Is recurrent and causes death in about 20% • Present with fever, cough, dyspnea, tachypnea, tachycardia, mild chest pain, cyanosis, respiratory distress
Opportunistic Infections cont. • TB: 4% with AIDS develop • Can be caused by reactivation of a previous infection • May be new, primary disease • Has a more rapid progression, diffuse infiltrates, and disseminated disease • Affects bone marrow, joints, liver, spleen, CSF, skin, kidneys, GI tract, lymph nodes, brain • Present with cough, purulent sputum, fever, fatigue, weight loss, lymphadenopathy
Opportunistic Infections cont. • Candiasis • Common, opportunistic fungal infection • Oral thrush or esophagitis • Often first indication of progression to AIDS • Difficulty swallowing, substernal pain or burning (increases with swallowing) • Women: vaginal candidiasis frequent and often recurrent
Opportunistic Infections cont. • Mycobacterium Avium Complex (MAC) • 25% of AIDS clients • Late in course of the disease • CD4 counts less than 50/mm3 • More common in women than men • Found in food, water and soil • Present with fever, chills, weakness, night sweats, abd pain, diarrhea, weight loss • Usually disseminated disease (any or all organs)
Other Infections • Herpes virus • CMV • Affects the retina, GI tract, lungs • Herpes simplex, or zoster • Toxoplasmagondii and cryptococcusneoformans affect CNS • Toxoplasmosis: encephalitis, changes in mental status • Cryotococcus: lungs • Cryptosporidium: protozoon: GI tract diarrhea • Women: PID
Secondary Cancers • Kaposi’s Sarcoma (old man’s cancer) • Late HIV disease • Survival time: 18 months maximum • See primarily face (nose) and pinnae of ears • Visceral disease: GI tract, lungs, lymphatic’s • Lymphoma’s (aggressive tumors) • Lymphocyte’s, lymph nodes, spleen, bone marrow • Non-Hodgkin’s, primary lymphoma of brain • Cervical Cancer: Pap smear every 6 months
Pediatric Manifestations • Neonate is asymptomatic at birth • Onset of AIDS shorter in children • Gram negative sepsis and prematurity primary causes of mortality in HIV + babies • Risk factors: prematurity, SGA, FTT • Signs and symptoms may occur within days • Early infancy: enlarged spleen/liver, swollen glands, recurrent URI/LRI, UTI’s, oral candidiasis, loss of achieved milestones
Pediatric Manifestations cont. • Within 2 years from infection develop conjunctivitis, ear infections, tonsillitis • With disease progression: infections with Streptococcus, Haemophilusinfluenzae, Salmonella, PCP • Develop lymphoma, lymphocytic interstitial pneumonitis, encephalopathy • Developmental delays, decreased motor functioning
Collaboration • The most vital strategy is prevention • Goals of care for client with HIV disease • Early identification of the infection • Promoting health maintenance to prolong the asymptomatic period as long as possible • Prevent opportunistic infections • Treat the complications of the disease • Provide emotional and psychosocial support
Nursing • Education on using one pharmacy for meds • Educate the community on prevention • Provide support to clients • Educate public on standard precautions in handling blood and body fluids • Limit exposure to infectious diseases when HIV +
Diagnostic Tests • To detect infection with HIV and monitor client’s disease and immune status • Rapid diagnostic tests: immediate results • Requires further testing to confirm a diagnosis • ELISA: most widely used • Tests for HIV antibodies, not the virus itself • Can have negative result in the early course of the disease • 99.5% sensitivity 13 weeks after infection
Diagnostic Tests cont. • Positive result: retest using different method • Western Blot antibody testing • More reliable than ELISA • More time-consuming • More expensive • Combined with ELISA: greater than 99.9% reliability • Clients blood is mixed with HIV proteins: if antibodies are present an antigen-antibody reaction will occur
Diagnostic Tests cont. • HIV viral load tests: levels correlate with disease progression and response to antiviral medications • 5,000-10,000 indicate the need for treatment • CBC: to detect anemia, leukopenia, thrombocytopenia • CD4 cell count: to monitor disease and guide therapy • Do every 3-6 months once diagnosed
Other Diagnostic tests • Blood culture for HIV: rarely done • Immune-complex-dissociated p24 assay • Indicates active reproduction of HIV and tends to be positive before seroconversion • TB skin test • MRI for brain lymphomas • Culture and sensitivity: infections • PAP smears
Pediatric Testing • ELISA and Western Blot: cannot distinguish between maternal and infant antibodies • May take up to 18 months to form their own antibodies • Preferred test: DNA polymerase chain reaction • Within 48 hours from birth • Do not use umbilical core blood • Acid associated p24 antigen used in infants older than one month
Pediatric Testing cont. • Second test at 1-2 months • Third test at 2-4 months • Infection + if two out of three are positive • Confirm absence at 12-18 months with a negative HIV antibody assay • PCR: if negative at birth, retest at 1-2 month, 3-6 months, 15 and 18 months • With two negative tests: ELISA at 12,15, 18 mos • CBC and CD4 counts at 3-6 months
Pharmacologic Therapies • HAART: three antiretroviral agents • Zidovudine (Retrovir, AZT) • An NRTI: nucleoside reverse transcriptase inhibitor • An NNRTI: nonnucleoside reverse transcriptase inhibitor • PI’s: protease inhibitors • Term infants: AZT 2mg/kg po every 6 hours for 6 weeks • If infant HIV + use multidrug antiretrovirals
Pharmacologic Therapies cont. • To suppress the infection itself • Decrease symptoms and prolong life • To provide prophylaxis of opportunistic infections • Stimulate hematopoietic response • To treat opportunistic infections and malignancies • Effectiveness is monitored by viral load and CD4 counts
Pharmacologic Therapies cont. • Positive results: reduced viral load and CD4 counts above 350/mm3 • Treatment recommended when CD4 falls below 200/mm3 • Do not initiate therapy in asymptomatic clients with higher CD4 levels • HARRT: 3-4 antiretrovirals • Reduces incidence of drug resistance and increase the likelyhood of decreasing viral loads and symptoms
Pharmacologic Therapies cont. • Triple combination drug: Trizivir • $1,030 per month • Does not include preventative/currative AB’s • Less than perfect adherence to therapy • Multiple meds throughout day • Physical changes from therapy: increased fat deposition in breast, midsection, neck, atrophy in face, buttocks, extremities • Labs: increase LDL’s and triglycerides, insulin resistance