Download
1 / 25
270 likes | 532 Vues
Efficacy of LLLT and Exesices After Hand Flexor Tendon Repair. Ahmed Barakat , PhD lecturer of orthopedic physical therapy. Introduction. Flexor tendon injury has long been recognized as a difficult problem in hand surgery.

E N D
Efficacy of LLLT and Exesices After Hand Flexor Tendon Repair
Introduction • Flexor tendon injury has long been recognized as a difficult problem in hand surgery. • Muscle atrophy, joint stiffness, osteoarthritis, infection, skin necrosis, ulceration of joint cartilage and tendocutaneous adhesion are familiar complications produced by prolonged immobilization of surgically repaired tendon ruptures. • Loss of active motion in the digits results in significant morbidity.
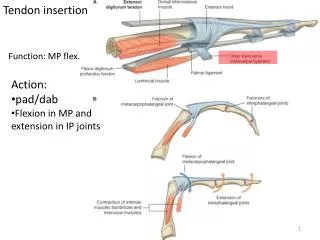
Introduction • These problems become more pronounced in zone II where the tendons travel through a fibro-osseous canal along the palmar aspect of the digits. • Zone II is located between the origin of the flexor sheath in the palm (distal palmar crease) and the insertion of the flexor digitorumsuperficialis tendon on the middle phalanx ).
Introduction • Unfortunately injuries in zone II are the most frequent injuries in the hand and carry the most severe prognosis. • The functional outcome is poorer and the complication rate is greater than that associated with injury in other zones. • It has been termed no man’s land because the healing tendon tends to adhere to its fibro-osseous tunnel.
Introduction • Tendon repair and subsequent immobilization is frequently complicated by postoperative stiffness secondary to inflammation and peritendinous adhesions and tissue edema. • Restoration of normal hand function following flexor tendon repair requires reestablishment not only the continuity of the tendon fibers, but also of the gliding mechanism between the tendon and its surrounding structures
Modulation of the tendon healing process remains a challenging problem. Despite remodeling, biochemical and mechanical properties of healed tendon tissue, it never matches those of intact tendon . • Low Level Laser Therapy (LLLT) has gained a considerable attention for enhancing tissue repair in a wide spectrum of applications.
Tissue healing is a complicated series of processes which consists of three overlapping processes: a. Inflammation b. proliferative stage c. Remodelling. .
A. Inflammation • characterized by vasodilatation and oedema formation. • A variety of cells arrive at the wound site e.g. Neutrophils, Macrophages, Lymphocytes, Platelets • bio-chemical mediators are important: a. Heparin → prevent occlusion of capillary blood flow b. Histamine → vasodilatation → heat and redness c. Bradykinin, Serotonin , and Prostaglandin → increase capillary membrane permeability → pain and swelling
B. proliferative stage • is the proliferative stage of repair, also comprising fibroplasia and angiogenesis C. Remodelling • is the establishment of an equilibrium between collagen formation and lysis, resulting in the constant reshaping of the scar over several months.
Laser physicsElectromagnetic spectrum • LLLT = a range of electromagnetic radiation of various wave lengths from 600- 1000 nm including both visible (red) radiation at the lower end of the visible range and invisible (near infrared) radiation.
wavelengths associated with: Visible red laser (He-Ne) = 632.8 nm is recommended for superficial conditions, Infrared (Ga-As) = 904 nm for deeper musculoskeletal structure
Assessment procedures • Maximum grip strength Was measured 3 weeks and 3 months postoperatively by the hand dynamometer.
Assessment procedures 2. ROM Was measured 3 weeks and 3 months postoperatively TAM = active PIP + DIP flex. – ext. lag
Treatment procedures: 1. accelerates inflammation, 2. promotes fibroblast proliferation, 3. quicken bone repair and remodeling, 4. encourages revascularization of wounds and 5.increased tensile strength during wound healing 6. stimulate DNA in damaged cell tissue. 7. kill the pain. overall accelerates tissue repair 1- Laser therapy
2- therapeutic exercises • All the patients will be treated by therapeutic exercises 3 sessions weekly for 12 weeks for total of (36) sessions. • All exercises done for three sets of 10 repetitions. • Patients will be instructed to do exercises at home, three times daily till three weeks
First 2 weeks • The hand will be splinted with posterior plaster slab • 30º wrist flexion, • 45º MCP joint flexion, • full IP joint extension • Hand kept elevated by a shoulder sling until the slab was removed at three weeks
5th day postoperatively • Splint was removed every session • passive fingers flexion and active extension for all fingers together • Passive flexion and extension for PIP and DIP joints separately
3rd and 4th week Active assisted finger flexion exercises Active wrist flexion and extension while fingers are flexed Active fingers flexion up to 1/3 of the range while wrist in neutral position
5th week Active finger flexion to ½ of the range Active wrist flexion and extension while fingers extended Passive finger full extension
6th week Active fingers flexion up to 2/3 of the range 7th and 8th week Full active free fingers flexion Isolated active finger flexion
9th to 10th week Isolated active finger flexion against mild to moderate resistance
11th to 12th week • Tendon gliding exercises: • Hook fist • Straight fist • Full fist