Download
1 / 1
10 likes | 93 Vues
How accurate are electronic blood loss records and do mistakes matter? Annette Briley 1 Henrietta Ballard 2 Graham Tydeman 3 Paul Seed 2 Jane Sandall 2 Rachel Tribe 2 and Susan Bewley 1 1 Guys and St Thomas’ NHS Foundation Trust, 2 King’s College London, 3 Forth Park Hospital, NHS Fife.

E N D
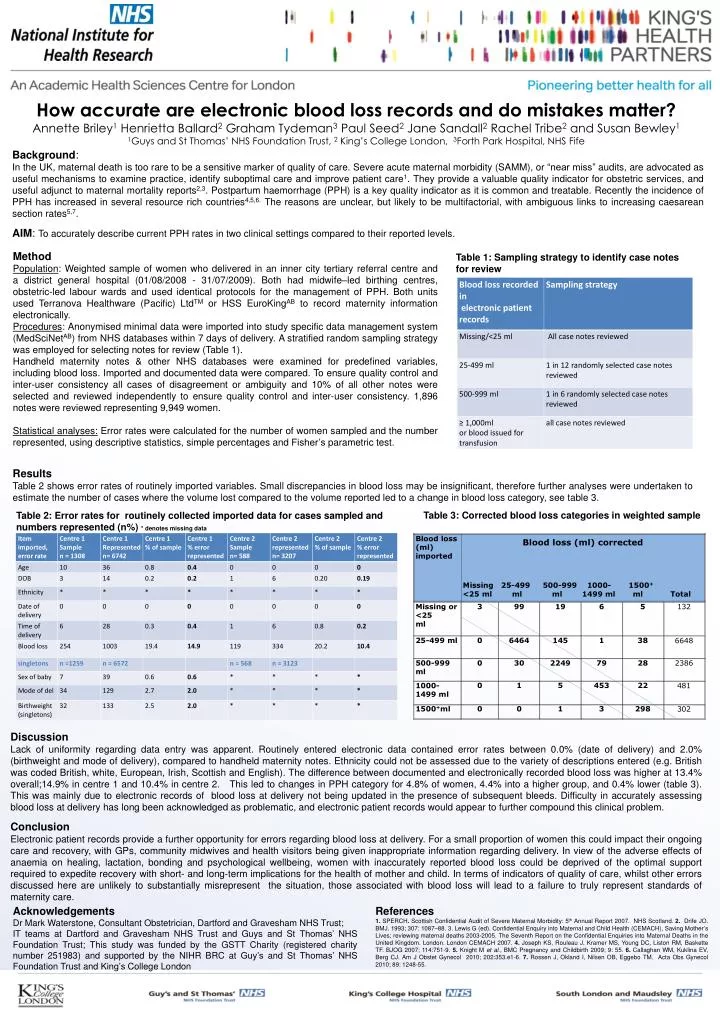
How accurate are electronic blood loss records and do mistakes matter? Annette Briley1 Henrietta Ballard2 Graham Tydeman3 Paul Seed2 Jane Sandall2 Rachel Tribe2 and Susan Bewley1 1Guys and St Thomas’ NHS Foundation Trust, 2 King’s College London, 3Forth Park Hospital, NHS Fife Background: In the UK, maternal death is too rare to be a sensitive marker of quality of care. Severe acute maternal morbidity (SAMM), or “near miss” audits, are advocated as useful mechanisms to examine practice, identify suboptimal care and improve patient care1. They provide a valuable quality indicator for obstetric services, and useful adjunct to maternal mortality reports2,3. Postpartum haemorrhage (PPH) is a key quality indicator as it is common and treatable. Recently the incidence of PPH has increased in several resource rich countries4,5,6. The reasons are unclear, but likely to be multifactorial, with ambiguous links to increasing caesarean section rates5,7. AIM: To accurately describe current PPH rates in two clinical settings compared to their reported levels. Method Population: Weighted sample of women who delivered in an inner city tertiary referral centre and a district general hospital (01/08/2008 - 31/07/2009). Both had midwife–led birthing centres, obstetric-led labour wards and used identical protocols for the management of PPH. Both units used TerranovaHealthware (Pacific) LtdTM or HSS EuroKingAB to record maternity information electronically. Procedures: Anonymised minimal data were imported into study specific data management system (MedSciNetAB) from NHS databases within 7 days of delivery. A stratified random sampling strategy was employed for selecting notes for review (Table 1). Handheld maternity notes & other NHS databases were examined for predefined variables, including blood loss. Imported and documented data were compared. To ensure quality control and inter-user consistency all cases of disagreement or ambiguity and 10% of all other notes were selected and reviewed independently to ensure quality control and inter-user consistency. 1,896 notes were reviewed representing 9,949 women. Statistical analyses: Error rates were calculated for the number of women sampled and the number represented, using descriptive statistics, simple percentages and Fisher’s parametric test. Table 1: Sampling strategy to identify case notes for review Results Table 2 shows error rates of routinely imported variables. Small discrepancies in blood loss may be insignificant, therefore further analyses were undertaken to estimate the number of cases where the volume lost compared to the volume reported led to a change in blood loss category, see table 3. Table 3: Corrected blood loss categories in weighted sample Table 2: Error rates for routinely collected imported data for cases sampled and numbers represented (n%) * denotes missing data Discussion Lack of uniformity regarding data entry was apparent. Routinely entered electronic data contained error rates between 0.0% (date of delivery) and 2.0% (birthweight and mode of delivery), compared to handheld maternity notes. Ethnicity could not be assessed due to the variety of descriptions entered (e.g. British was coded British, white, European, Irish, Scottish and English). The difference between documented and electronically recorded blood loss was higher at 13.4% overall;14.9% in centre 1 and 10.4% in centre 2. This led to changes in PPH category for 4.8% of women, 4.4% into a higher group, and 0.4% lower (table 3). This was mainly due to electronic records of blood loss at delivery not being updated in the presence of subsequent bleeds. Difficulty in accurately assessing blood loss at delivery has long been acknowledged as problematic, and electronic patient records would appear to further compound this clinical problem. Conclusion Electronic patient records provide a further opportunity for errors regarding blood loss at delivery. For a small proportion of women this could impact their ongoing care and recovery, with GPs, community midwives and health visitors being given inappropriate information regarding delivery. In view of the adverse effects of anaemia on healing, lactation, bonding and psychological wellbeing, women with inaccurately reported blood loss could be deprived of the optimal support required to expedite recovery with short- and long-term implications for the health of mother and child. In terms of indicators of quality of care, whilst other errors discussed here are unlikely to substantially misrepresent the situation, those associated with blood loss will lead to a failure to truly represent standards of maternity care. . Acknowledgements Dr Mark Waterstone, Consultant Obstetrician, Dartford and Gravesham NHS Trust; IT teams at Dartford and Gravesham NHS Trust and Guys and St Thomas’ NHS Foundation Trust; This study was funded by the GSTT Charity (registered charity number 251983) and supported by the NIHR BRC at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London References 1. SPERCH. Scottish Confidential Audit of Severe Maternal Morbidity: 5th Annual Report 2007. NHS Scotland. 2.Drife JO. BMJ. 1993; 307: 1087–88. 3. Lewis G (ed). Confidential Enquiry into Maternal and Child Health (CEMACH), Saving Mother’s Lives; reviewing maternal deaths 2003-2005. The Seventh Report on the Confidential Enquiries into Maternal Deaths in the United Kingdom. London. London CEMACH 2007. 4. Joseph KS, Rouleau J, Kramer MS, Young DC, Liston RM, Baskette TF. BJOG 2007; 114:751-9. 5. Knight M et al., BMC Pregnancy and Childbirth 2009; 9: 55. 6. Callaghan WM, Kuklina EV, Berg CJ. Am J ObstetGynecol 2010; 202:353.e1-6. 7.Rossen J, Okland I, Nilsen OB, Eggebo TM. Acta Obs Gynecol 2010; 89: 1248-55.