Download
1 / 22

E N D
M.Prasad Naidu MSc Medical Biochemistry, Ph.D.Research Scholar Jaundice
Clinical marker of defect in metabolism &/or excretion of bilirubin. ER task to initiate lab eval or imaging studies to identify cause and determine admission or outpt therapy. Jaundice
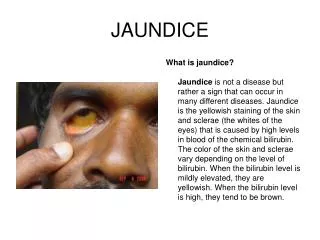
Yellow discoloration of sclera, skin, mucous membranes due to deposition of bile pigment Clinically detected with serum bilirubin 2-2.5mcg/dL or (2 times nl) Pathophysiology
The breakdown product of Hgb from injured RBCs and other heme containing proteins. Produced by reticuloendothelial system Released to plasma bound to albumin Hepatocytes conjugate it and extrete through bile channels into small intest. What is bilirubin?
Overproduction by reticuloendothelial system Failure of hepatocyte uptake Failure to conjugate or excrete Obstruction of biliary excretion into intestine What causes bilirubin?
Unconjugated vs. Conjugated • Unconjugated • production exceeds ability of liver to conjugate • Ex. Hemolytic anemias, hemoglobinopathies, in-born errors of metab., transfusion rxn. • Conjugated • Can produce but not excrete • Metabolic defect • Intra- or extrahepatic obstruction
Careful history and PE Family history (Gilbert, Rotor, Crigler-Najjar, Dubin-Johnson, Sickle Cell) Healthy young person with fever, malaise, myalgias = viral hepatitis (try to locate source) Clinical Features
Gradually develops symptoms = hepatic/bile duct obstruction (consider ETOH liver dz/cirrhosis) Develops acutely with abd pain = acute cholangitis 2° to choledocholithiasis Clinical Features
Painless jaundice in older person with epigastric mass & weight loss = biliary obstruction from malignancy Hepatomegaly with pedal edema, JVD, and gallop = CHF Clinical Features
Laboratory Tests • Serum bilirubin level (total and direct) • Liver aminotransferase levels • Alk. Phos • U/A for bilirubin and urobilogen • CBC • PT • Other labs pertinent to history • Coombs test • Hgb electrophoresis • Viral hepatitis panel • U/S Gallbladder
Hemodynamically stable, new-onset jaundice, no evidence of liver failure or acute biliary obstruction discharge with follow up If one of above violated admission with surgery consult Disposition
Tintanalli Chapter 85 Pages 561-566 Cholecystitis and Biliary Colic
1) Biliary Colic 2) Cholecystitis 3) Gallstone pancreatitis 4) Ascending cholangitis Biliary Tract Emergencies Related to Gallstones
Most gallstones are asymptomatic Usually seen in obese females 20-40 yoa and pregnancy (Remember fat, fertile, flatulent, female, forty) Associated with upper abdominal pain Gallstones
Uncommon in children (seen with hemolytic d/o, idiopathic, cystic fibrosis, obesity, ileal resection, long term use of TPN) • Elderly • 14-27% symptomatic gallstone dz. • More likely biliary sepsis/gangrenous GB • perioperative morbidity • Mortality rate 19% Gallstones
Familial • Asian descent • Chronic biliary tract infections • Parasitic infections (ascaris lumbricoides) • Chronic liver dz (ETOH) • Chronic intravasular dz (Sickle Cell, Hereditary Scherocytosis) • Hepatitis A, B, C, E • HIV • Herpesvirus Gallstone Risk Factors
Bile • Manufactured & secreted from hepatocytes GB storage in canaliculi, ductiles, & bile ducts bile ducts enlarge form R and L hepatic ducts form common hepatic duct joins cystic duct from GB to form CBD Ampulla of Vater duodenum Pathophysiology
Release of bile stimulated by cholecystokinin secreted from small int. mucosal cells when fats & AA enter duodenum Pathophysiology
Symptomatic cholelithiasis = stone migration from GB into biliary tract with eventual obstruction obstruction of hollow viscus pain, nausea & vomiting acute cholecystitis Pathophysiology
E. coli/Klebsiella-70% Enterococci-15% Bacteroides-10% Clostridium-10% Group D Strep Staphylococcal species Pathogens Involved in AcuteCholecystitis
Overlap of s/s of PUD, gastritis, GERD, nonspecific dyspepsia RUQ pain Upper abd/epigastric pain Radiation to L upper back Pain persisant lasting 2-6h Clinical Features