Download
1 / 44
790 likes | 2.38k Vues
Surgical Anatomy Thyroid and Parathyroid Glands. Bastaninejad Shahin MD, ORL&HNS, TUMS, Amiralam Hospital. Presentation outlines. Thyroid Gland: General measures Vascular supply Important proximities Surgical approaches and important Landmarks Parathyroid glands: General measures

E N D
Surgical Anatomy Thyroid and Parathyroid Glands BastaninejadShahin MD, ORL&HNS, TUMS, Amiralam Hospital
Presentation outlines • Thyroid Gland: • General measures • Vascular supply • Important proximities • Surgical approaches and important Landmarks • Parathyroid glands: • General measures • Surgical localization • Thyroid Function Tests
General measures • Two lateral lobes connected with isthmus • Total weight is about 15 to 25 g • Each lobe: 4 x 1.5 x 2cm(height/width/depth) • Extends from C5 to T1 vertebra • Isthmus is over 2nd & 3rd tracheal ring • Approximately 40% of patients have a pyramidal lobe that arises from either lobe or the midline isthmus
General measures... • Cervical Fascia: • True Thyroid Capsule • Surgical Capsule • Berry’s Ligament (connecting the lobes of the thyroid to the cricoid cartilage and the first two tracheal rings) • Surgical Approaches regarding to the Fascia: • IntracapsularThyroidectomy • Extracapsular Thyroidectomy • Combine!?
Vascular Supply • Two pairs of arteries • Three pairs of veins • Connecting vessels within the thyroid true capsule • In less than 10%, there is a midline arterial supply to the gland, named as Thyroid Ima artery
About 12cm About 5-6cm
Surgical approaches and Landmarks • The course of the inferior laryngeal nerve is highly variant • Incidence of nerve paralysis is three to four times greater in cases in which the recurrent nerve was not localized compared with cases in which it was • Try to seek, expose and identifying the nerve, instead of avoiding it! • Extracapsular approach with nerve identification is the method of choice
The most common course of the nerve is within TE Groove (48.5% - not depicted here) Incidence is more higher in Revision cases 42.2% 5.4% 3.9%
Surgical approaches and Landmarks • Lateral Approach • Inferior Thyroidal Artery • Tubercle of Zuckerkandl (ZT) • Inferior Approach • Lore’s triangle • Tracheoesophageal Groove • Superior Approach • Posterolateral aspect of the Cricoid • Berry’s ligament • Inferior border of the inferior Constrictor • Inferior horn of the thyroid cartilage
...Lateral Approach • Used most commonly • RLN is identified typically at the thyroid midpole level (less nerve dissection required) • This approach is less useful for Revision
...Inferior Approach • Used for Revision cases and Goiter surgery (not substernal) • Problem: Longer nerve dissection and probability of Parathyroid glands ischemia • Benefit: nerve will be find before any extralaryngeal branching
...Superior Approach • Used for large substernal Goiters • Nerve is at the lower edge of the lateral aspect of the cricoid cartilage • Nerve should be identified just caudal to the lowest fibers of the inferior constrictor
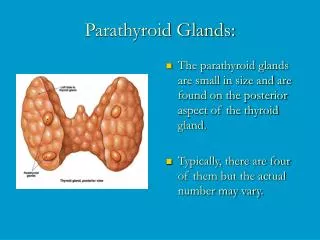
General measures • Two pairs: Superior and Inferior • Weight is about 50 to 70 mg • Size 5 x 3 x 1 mm • Color of normal parathyroid glands ranges from yellowish brown to reddish brown • 87% there are four glands (super numerary glands are usually in the mediastinum or thymus gland) • Their Arterial supply is usually from Inferior Thyroid artery (80%)
Surgical Localization • Superior Parathyroid Glands • 80% they are at the cricothyroid junction approximately1 cm cranial to the juxtaposition of the recurrentlaryngeal nerve and the inferior thyroid artery. • Ectopic glands: it cloud be intrathyroid, paraesophageal, retroesophageal and mediastinal (posterior superior compartment)
...Surgical Localization • Inferior Parathyroid Glands: • More variable location • More than 50% of the inferiorparathyroid glands are situated near the lower poleof the thyroid gland • Ectopic glands: it could be situated in thyrothymic ligament (28%) or mediastinum (Anterior superior compartment)
ThyroidFunction Tests • TSH • FT4, (T4) • FT3, (T3) • Thyroglobulin • Thyroid stimulating immunoglobulin (TSI) • Antithyroid peroxidase antibodies (Anti-TPO) • RAIU
Serum TSH • Single best initial test of the thyroid function • Normal range 0.5 – 5.0 mU/L • If TSH alone is the first line test, what diagnoses will be missed? • Pituitary disease or tumors • Hypothyroidism develops within 12 months of treatment for thyrotoxicosis (the TSH value remains suppressed) • Thyroid hormone resistancy • Non-thyroidal illness (NTI) • Pregnancy • In these cases testing of free thyroid hormones is recommended in addition to the TSH assay (FT4 + TSH)
Screening Recommendations • Various societies and authors disagree about population-based screening • There are insufficient evidences to recommend for or against routine screening for thyroid disease in adults. • The AAFP recommends screening high-risk populations: • women with a family hx of thyroid disease • women >35 y.o. • pregnant women • abnormal physical exam • diabetic patients • Hx of autoimmune disorder • The American Thyroid Association (ATA) recommends screening start at age 35 (and q 5 years after that)
Serum T4 • Serum total T4 assays measure both bound and unbound (“free”) T4 • Levels are high in approximately 90% of hyperthyroid patients and low in approximately 85% of hypothyroid patients.
Serum Free T4 • FT4 is measured by equilibrium dialysis techniques or estimated indirectly by calculation of free-thyroxine index (FTI) • FT4 assay is preferred test with TSH or when TSH is high
T3, Free T3, and rT3 • T3 • binding protein dependent • Levels can be misleading in patients with acute illness, cirrhosis, uremia, or malnutrition • FT3 • Useful to distinguish T3 toxicosis from subclinical thyrotoxicosis • When TSH is low, a free T3 assay should be obtained • Measurement of fT3 is not indicated in hypothyroidism • Reverse T3 (rT3) - increased in NTI - it is an inactive hormone - helpful to exclude central hypothyroidism
Other Ancillary Tests • Serum thyroglobulin • produced and released by thyroid gland • marker for recurrent thyroid cancer • differentiate Graves disease from factitious thyrotoxicosis • Serum thyroid-stimulating immunoglobulin (TSI) • Expensive test • Graves’ disease. • Antithyroid peroxidase antibodies (Anti TPO) • organ-specific and sensitive. • Hashimoto’s thyroiditis • predict overt hypothyroidism (use in subclinical hypothyroidism)
Other… • Radioactive iodine uptake (RAIU) • A very high RAIU is seen in individuals whose thyroid gland is overactive (hyperthyroidism) • A low RAIU is seen when the thyroid gland is underactive (hypothyroidism)