Download
1 / 58
830 likes | 2.1k Vues
Narrow Complex Tachycardias. Moritz Haager PGY-5. Objectives. Develop an approach Review treatment options Dispositon decisions. Perspective. SVT Broad umbrella term for any tachycardia originating above the ventricles Variable underlying mechanisms but basically one Tx approach

E N D
Narrow Complex Tachycardias Moritz Haager PGY-5
Objectives • Develop an approach • Review treatment options • Dispositon decisions
Perspective • SVT • Broad umbrella term for any tachycardia originating above the ventricles • Variable underlying mechanisms but basically one Tx approach • Ranges from physiological pathological, and benign dangerous • Occurs in all age groups • Clinical presentation from asymptomatic shock / CHF When presented with an undifferentiated presentation with a broad DDx and variability in outcome you need an APPROACH
Why should we care? • Morbidity & Mortality • Patient discomfort & anxiety • Syncopal events (falls) ~15% • Risk of sudden cardiac death w/ accessory pathway driven arrhythmias • Tachycardia-mediated cardiomyopathy • LV dilatation w/ impaired LV function
Approach to Tachycardia • Stable or unstable? • Assess ABC’s, O2, IV, monitors, crash cart to bedside • In general if unstable, give’m juice • Narrow or wide QRS? • Regular or irregular? • Look at the P waves • Relationship to QRS • P wave axis / rate • P wave morphology(ies) • What is the trigger / underlying cause?
Step 1: Stable or Unstable? • Not always black & white • Continuum from stable compensated decompensated shock arrest • Stability determined by big picture: • Symptoms, signs, & vitals • Cardio-respiratory reserve • Age • Co-morbidities • Be prepared • Any dysrhythmia could potentially deteriorate • All therapies are potentially pro-arrhythmic
Step 2: Narrow or wide? • Measure widest QRS on ECG • Adults: wide = >0.12 sec (3 small boxes) • Kids <8yo: wide = >0.08 sec (2 boxes)
Step 3: Regular or Irregular? • Use calipers or paper • Irregularity can be subtle, esp at fast rates • Generally • Irregular rhythms originate ABOVE the AV node • VT is almost never irregular
Step 4: Look at the P waves • P waves present? • Is there a P before every QRS? • What is the relationship b/w the P and the QRS? • What is the P wave rate? Ventricular rate? • Is the P wave coming from the SA? • N axis: upright in II, negative in aVR • Is there >1 distinct P wave morhology?
Diagnostic Trick: 50 mm/s ECG Tracings • Comparsion study of 8 EP’s • Given 45 ECG’s of NCT’s printed at 25 mm/s & asked to give Dx & Tx plan • 2 wks later given same ECG’s printed at 25 & 50 mm/s & asked to give Dx & Tx • Results • 50 mm/s increased diagnostic accuracy from 63 to 71%, P=0.002 • J Emerg Med 2002; 22: 123–126
Final Categorization • Narrow Complex Tachycardias • Regular w/ P’s • = sinus, a. flutter w/ constant block, Focal atrial tachycardia, AVNRT, junctional tachycardia • Irregular w/ P’s • = MAT, a. flutter variable block • Regular, no P’s • = AVRT, AVNRT • Irregular, no P’s • = a. fib • Wide Complex Tachycardias Tx w/ AV nodal blockers Rate control +/- rhythm control
Step 5: Underlying Causes • HIS DEBTS • H – Hypoxia • I – Ischemia / infarction • S – Sympathetic excess • Hyperthyroid, CHF, pheochromocytoma, excercise • D – Drugs • Anti-arrhythmics, cocaine, amphetamines, caffeine, etc • E – Electrolytes • K+, Ca2+, Mg2+ • B – Bradycardias • Eg. Sick sinus syndrome • T – Thyroid disease • S – Stretch • Hypertrophy / dilation of atria & ventricles (CHF, valvular Dz) Preciptants vary w/ age, sex, co-morbidities, etc
Clinical Presentations • Typical Sx • Palpitations 96% • “Dizziness” 75% • Dyspnea 47% • Fatigue 23% • Chest pain 35% • Diaphoresis 17% • Nausea 13% • Neck pounding said to be pathogonomonic
Case • 27 yo M w/ palpitations & dyspnea • NCT at 160 on ECG c/w PSVT • Also tells you he has been “pissin’ like a racehorse” • Does he have diabetes?
Polyuria in PSVT • Loss of AV synchronization • Atrial contraction against closed AV valves • Elevated atrial pressure & atrial stretch • Release of atrial natriuretic peptide polyuria NB: This is trivia – absence of polyuria does NOT exclude Dx of PSVT and you should still check at least a urine for glucose
Case • 3 mo F w/ dyspnea & wheeze • T 40.5oC, P 190, RR 60, SpO2 88% • Mod resp distress on exam w/ wheezes & crackles bilaterally • Is this just sinus tachycardia from her fever?
Tachycardia & Fever • Prospective observational study of 490 infants <1 yo • Measured HR & rectal temp in calm, quiet kids w/o evidence of serious illness • Analyzed relationship b/w HR & temp w/ multivariate linear regression • Results • HR increased ~10 bpm for every 1oC rise in infants b/w 2 -12 mo • Ann Emerg Med. 2004;43:699-705
Tachycardias: Mechanism • Reentry • 50-80% of NCT’s • Abrupt on-/off-set • Do well w/ electricity • Enhanced automaticity • Typically catecholamines, drugs, lytes, ischemia • Gradual on-/off-set • Not likely to respond to electricity; Tx underlying cause • Triggered dysthythmias • Interruption of repolarization by afterdepolarizations • Ischemia, drugs, lytes, catecholamines • Not likely to respond to electricity; Tx underlying cause E.g. Torsades IV magnesium
Maximal sinus tach • 220 – age = maximum HR • 220 -80 = 140 • Unlikey this is just sinus tach
Regular NCT: DDx • P waves present: • Sinus tachycardia • Atrial Flutter • AVNRT • AVRT • Focal Atrial Tachycardia • No P-waves • AVRT • AVNRT • Junctional Tachycardia Consider under PSVT as can be impossible to differentiate on ECG; Tx generally the same
AV nodal reentrant tachycardia Most common PSVT (>60%) Dual AV nodal physiology 2 separate conduction paths in AV node Fast pathway Slow pathway Allow for re-entry circuit w/in AV node Atrioventricular reentrant tachycardia accessory pathway(s) (AP) = Tracks of conducting tissue outside of AV node, connecting atria & ventricles Re-entry circuit formed by AP & AV node (WPW) 2 or more separate AP’s (bypass AV node completely) AVNRT vs. AVRT
AVNRT • “Typical” AVNRT – = 90-95% • Anterograde conduction down slow pathway • Retrograde conduction up fast pathway • If P waves seen RP < PR interval ATRIA VENTRICLES “Atypical” AVNRT is the reverse of what is pictured here
2 types of AP “concealed” = capable of retrograde conduction only “manifest” = allow anterograde +/- retrograde conduction See “pre-excitation” on ECG AVRT
WPW (Wolf-Parkinson-White) PR <120 msec QRS >100 msec Delta waves in some leads LGL (Lown-Ganong-Levine) PR <120 msec Preexcitation Syndromes
Orthodromic SVT Anterograde via AV & returns via accessory tract Uses normal conduction system therefore get narrow complex tachycardia WPW & SVT Orthodromic makes up 90-95% of WPW SVT’s
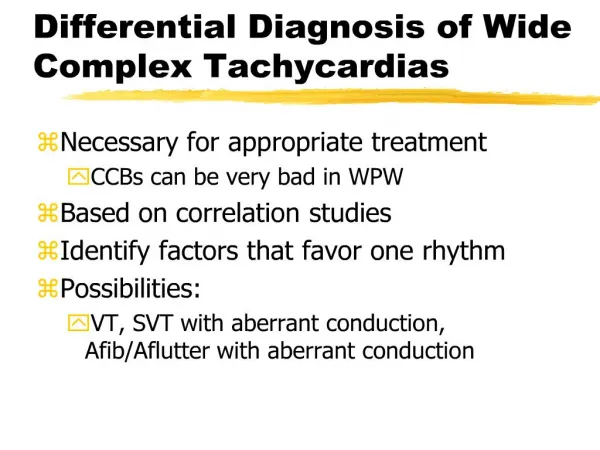
WPW & SVT • Antidromic SVT • Anterograde conduction from atria to ventricles via accessory path & retrograde flow through AV node • Wide complex tachycardia • Avoid AV nodal blockers • Use procainamide or cardiovert (5-10% of WPW SVT)
WPW & A Fib • IrregularWide complex tachycardia • May see capture & fusion beats • Common (~30% of WPW pts) & potentially life-threatening • AP w/ short refractory period & anterograde conduction near 1:1 conduction VF • 0.15 – 0.39% incidence of sudden cardiac death • Do NOT block AV node • Channels all impulses down AP & increases risk of VF • Use Procainamide or cardioversion
Predictors of Sudden Cardiac Death in WPW • Shortest pre-excited R-R interval during atrial fib <250 ms • Hx of symptomatic tachycardia • Multiple accessory pathways • Ebstein’s anomaly* • Blomström-Lundqvist et al. ACC/AHA/ESC Guidelines for Management of SVA ACC 2003; 42:1493–531 *= abnormal tricuspid valve regurgitation & RA enlargement
AVNRT vs. AVRT: Can you tell them apart • Helpful ECG findings • Pseudo R’ in V1 • Pseudo S in II, III, aVF • specific (but not sensitive) for AVNRT • ST elevation in aVR • RP >100 ms • ST depression ≥2mm • Suggest (not highly specific or sensitive) AVRT Bottom line = 12-lead lacks 100% accuracy but important to look because AVRT more serious Dx See Adam Osters talk July 22, 2004 for more detailed explanation
PSVT: Acute Treatment Summary • Unstable • DC cardioversion • Stable • 1) Vagal maneuvers (Class I/ level A) • 2) Adenosine (Class I/ level A) • 3) CCB’s (Class I/ level A) • 4) BB’s (Class IIb/ level C) • 5) Amiodarone (Class IIb/ level C) • 6) Digoxin (Class IIb/ level C) Blomström-Lundqvist et al. ACC/AHA/ESC Guidelines for Management of SVA JACC 2003; 42:1493–531
Cardioversion • Sedation • ?1 mg midaz + 100 mcg fentanyl • Energy Levels • PSVT:- 50 Joules • Atrial fibrillation: 200 Joules • Atrial flutter: 25-50 Joules • Orthodromic WPW: 50 Joules • Narrow Complex VT: 50-100 Joules
Adenosine • Actions • Coronary vasodilator • Transient SA & AV nodal blockade • Outward K+ current hyperpolarizes cells • Reflex catecholamine release & sympathetic discharge • T1/2 <10 sec; • Duration of action 30-40 sec
Adenosine: Adverse Effects • Hot flash / flushing ~25% • Dizziness ~20-50% • Chest pain / pressure ~20-40% • Dyspnea ~10-25% • Feeling of impending doom ~10% • Pro-arrhythmia / blocks ~10% >75% of pts will experience side effects w/ adenosine
Adenosine: Pro-arrhythmic Effects • Significant literature reports • A fib, VF, Transient sinus arrest / asystole, Torsades de pointes • Prospective observational ED study • 160 consecutive pts given adenosine • Overall 21 (13%) pts had pro-arrhythmic s/e • Prolonged AV block (>4sec) 11 (7%) • Atrial Fib 2 (1%) • Non-sustained VT 8 (5%) • All resolved spontaneously; no serious outcomes Euro J Emerg Med 2001; 8: 99-105
Pearls • Adenosine CAN convert some VT, • giving it to “diagnose” SVT w/ aberrancy is misguided • Wide & irregular – think WPW + A fib • NO AV nodal blockers • Amiodarone may not be ideal • Procainamide is the drug of choice
Adenosine: Drug Interactions • Theophylline • ↑’s dose requirement • Dipyridamole • ↓’s dose requirement • Carbamazepine • potentiates adenosine-induced heart block • CCB’s / BB’s • Potentiate hypotension & bradycardia
Adenosine Dosing • DBRCT of 201 pts w/ PSVT: • Adenosine Dose Conversion Rate • 3 mg 35.2% • 6 mg 62.3% • 9 mg 80.2% • 12 mg 91.4% • P<0.001 for all doses c/w placebo • All administered through PIV DiMarco et al. Ann Intern Med 1990; 113: 104-110
Practical Pearl • Adenosine administration • Want to get it in as fast as possible • Use 2 syringes w/ 18g needles • one w/ adenosine • Other w/ 10 cc NS • Put both needles into IV access port • Push the adenosine w/ one hand and… • …chase immediately w/ the NS w/ the other • NB: want an IV in the AC if at all possible
Adenosine via Central Line • Appears to have increased success rate • Observational study of 200 pts w/ PSVT induced in EP lab • found 99% success rate w/ 12 mg via femoral line • Strickberger et al. Ann Intern Med 1997; 127: 417-422 • Randomized Cross-over study of 30 pts given adenosine via PIV or central line • success rate w/ 3 mg was 77% when given via central line vs. 37% via PIV • McIntosh-Yellin et al. JACC 1993; 22:741–5 • Case reports of more severe S/E via central line (felt to be dose-related)
Case 4 • 31 yo F w/ PSVT • Vagal maneuvers fail • 6 mg adenosine IV no response • 12 mg adenosine IV slows down briefly • What now? Would you give her 18 mg of adenosine?
High Dose Adenosine • Background • ACLS: 6 mg, then 12 mg x2 if unsuccessful • FDA approves use up to 12 mg • Literature reports of uses up to 25 mg • What about higher doses? • Randomized cross-over comparison of of 31 pts w/ AVNRT/AVRT in EP lab given 12 & 18 mg adenosine via PIV • Non-significant increase in efficacy w/ 18 mg • 25/31 (81%) vs. 29/31 (94%); P = 0.103) • No significant increase in adverse effects • may have been underpowered to find difference Weismueller et al. Deutsche Med Wochenschrift 2000. 125: 961-69
Calcium Channel Blockers • 2nd line agents in PSVT • Verapamil • 1st dose: 2.5 – 5 mg IV over 2 min • 2nd dose (30 min later): 2.5 – 10 mg IV over 2 min (to max of 20 mg) • NB: CONTRAINDICATED in <1yo (risk of EMD), wide QRS, or hypotensive pts, CHF, or WPW • Diltiazem • 1st dose: 0.25 mg/kg IV over 2 min • 2nd dose (15 min later): 0.35 mg/kg IV over 2 min followed by gtt of 5-15 mg/h • Generally felt to be safer than Verapamil but same cautions apply
What about Verapamil? • RCT of 122 pts w/ PSVT treated w/ either adenosine or Verapamil • NS difference in conversion to NSR • 86.0% (52/60) vs. 87.1% (54/62), p=NS • Adenosine worked much faster • 34.2 +/- 19.5 sec vs. 414.4 +/- 191.2 sec, P < 0.0001 • Cheng KA Zhonghua Nei Ke Za Zhi 2003; 42(11): 773-6
Adenosine vs Verapamil DBRCT of 70 pts w/ PSVT DiMarco et al. Ann Intern Med 1990; 113: 104-110
Retrospective study of 106 pts w/ PSVT treated w/ adenosine or verapamil No sig difference in overall efficacy Logistic regression found Adenosine worked better w/ faster HR Verapamil had better success w/ slower HR Adenosine vs. Verapamil Interesting study, but hypothesis-generating at most; needs prospective, randomized investigation Euro Heart J 2004; 25: 1310–1317
Case • 78 yo F presents w/ NCT • Hx of PSVT – ECG looks identical • Had severe side effects w/ adenosine previously & refuses repeat • Does not want to be shocked either • When you ask for Verapamil the nurse points out her pressure is only 88/65 • What can you do?
Calcium pre-Tx to prevent CCB-induced hypotension • Verapamil = vasodilator + myocardial depressant • Get some decrease in BP (5-40 mm Hg) in up to 75% pts when given via IV route • No RCT’s looking at Ca2+ pre-Tx • 6 trials totalling 322 pts suggest pre-Tx blunts Verapamil-induced decrease in BP • Ca gluconate 1g IV over 5 min appears to be a reasonable choice • Ann Pharmacother 2000; 34: 622-9. NB: No studies exist on Ca2+ pre-Tx for IV Diltiazem
PSVT: Chronic Tx • Pts w/ frequent episodes / severe Sx • Drugs • CCB’s • B-blockers • Digoxin • Other antirhythmics • Pill-in-pocket approach • Dilitiazem 120 mg PO + propranolol 80 mg PO appears to work best • Rarely get hypotension or bradycardia • Decreases ED visits • Catheter ablation techniques in EP lab • Curative in >90% of pts – becoming 1st line May be reasonable to start in ED, but need reliable F/U Better left to cardiology or EP