Download
1 / 36
380 likes | 384 Vues
Diabetes and the Pharmacy Army. Philip Newland-Jones Consultant Pharmacist Diabetes and Endocrinology. Type 2 diabetes is a progressive disease associated with weight gain. Diagnosis. Hyperglycaemia. Time. Non-Diabetic Hyperglycaemia. Normal. Diabetes. Blood glucose. Weight gain.

E N D
Diabetes and the Pharmacy Army. Philip Newland-Jones Consultant Pharmacist Diabetes and Endocrinology
Type 2 diabetes is a progressive disease associated with weight gain Diagnosis Hyperglycaemia Time Non-Diabetic Hyperglycaemia Normal Diabetes Blood glucose Weight gain Insulin Production Insulin resistance Adapted from: Kendall D et al. Am J Med 2009;122:37–50 Beta Cell Function
Interventional Relationships Between Cholesterol, BP and HbA1c with CVD events(20) NNT for 5 years in order to prevent 1 CVD event 0.9% reduction in HbA1c 1 mmol/L reduction in cholesterol 10/5 mmHg reduction in BP For each variable, data shown are for a change corresponding to the mean change of the variable in intervention studies BP=blood pressure; CVD=cardiovascular disease; NNT=number needed to treat 20. Adapted from Yudkin JS et al (2010) Diabetologia53: 2079–85 https://link.springer.com/content/pdf/10.1007%2Fs00125-010-1864-z.pdf Accessed September 2017
Internal use only. Not for distribution Drug choice in T2DM 2005 Analogue prandial insulin1,6 Acarbose1 Analogue basal insulin1-5 Metformin1 TZDs1 NPH insulin1 Meglitinides1 SU drugs1 2017 2006 1946 Diabetes drugs (date of first authorisation) 1. White JR, Diabetes Spectrum 2014; 27(2): 82-86
Internal use only. Not for distribution Drug choice in T2DM 2017 U200 units/ml U300 units/ml Biosimilar First in class Follow-on drugs DPP-4i + SGLT-2i20 ⌘ GLP-1 RA + basal insulin21,22 ⌘ SGLT-2i + Metformin17-19 SGLT-2 inhibitor1, 16 DPP-4i + Metformin11-15 ⌘ DPP-4 inhibitor1, 10 GLP-1 RA 1x weekly1, 8, 9 GLP-1 RA 1x/2x daily1, 7 * Analogue prandial insulin1,5,6 * Analogue basal insulin1-4 2008 2014 2016 2006 2012 2010 2017 Acarbose1 Analogue basal insulin1 Metformin1 TZDs1 NPH insulin1 Meglitinides1 SU drugs1 Analogue prandial insulin1 2017 2006 1946 Diabetes drugs (date of first authorisation) 1. White JR, Diabetes Spectrum 2014; 27(2): 82-86 ⌘ = fixed-dose combination * = date of CHMP approval, Toujeo (Ref 4 ), Humalog 200 units/ml (Ref 6)
Goal of insulin development: approach endogenous insulin secretion by healthy pancreatic beta-cells Recombinant insulin + hyaluronidase Recombinant insulin + EDTA BioChaperone lispro Physiologically distributed insulin Fast-acting insulin aspart Trepostinillispro Rapid-acting insulin analogue 1996 Exubera inhaled insulin (withdrawn 2007) 2006 Short-acting 1920 1940 1960 1980 2000 2014–2015 Ultra-fast-acting First clinical use of insulin 1922 Biosynthetic human insulin 1982 Afrezza inhaled insulin 2015 1950 NPH insulin 2000 Long-acting insulin analogue 2013 Degludec 2015 Glargine U300 Long-acting Future 1953 Lente insulin PEGylated insulin (discontinued) Smart insulin 2015 Biosimilar glargine U100 EDTA, ethylenediaminetetra-acetic acid; NPH, neutral protamine Hagedorn • Adapted from Cahn et al. Lancet Diabetes Endocrinol2015;3:638–52 • Eli Lilly Patent Application 12 Nov 2015; Eli Lilly Press Release 4 Dec 2015; Novo Nordisk Capital Markets Day R&D update 19 Nov 2015
Treatment options in the management of type 2 diabetes BP: blood pressure; DPP-4: dipeptidyl peptidase-4;GLP-1: glucagon-like peptide-1; HDL: high density lipoprotein; LDL: low density lipoprotein; SGLT2: sodium-glucose co-transporter-2; TZD: thiazolidinedione; TG: triglycerides. 1. Adapted from Nathan DM et al. Diabetes Care. 2009;32:193–203; 2. Wulffele MG et al. J Intern Med. 2004;256:1–14; 3. Victoza (liraglutide) SmPC. Available at: https://www.medicines.org.uk/emc/medicine/21986 (accessed August 2017); 4. Jardiance (empagliflozin) SmPC. Available at: https://www.medicines.org.uk/emc/medicine/28973 (accessed August 2017); 5. Valentine V. Clinical Diabetes. 2012:30:151–155; 6. Phillips P et al. Diabetes Care. 2003;26:269–273; 7. Acarbose SmPC. Available at: https://www.medicines.org.uk/emc/medicine/27829(accessed August 2017); 8. Kurukulasuriya LR. and Sowers JR. Cardiovasc Diabetol. 2010;9:45; 9. The Cochrane Collaboration. Meglitinide analogues for type 2 diabetes mellitus (review); 10. Prandin (replaginide)SmPC. Available at: https://www.medicines.org.uk/emc/medicine/18980 (accessed August 2017); 11. Inzucchi SE. et al. Diabetologia. 2012;55:1577–1596.
Comparator – HbA1c & MPG Diabetes Care 2008 (8) 1473-8
Blood Glucose Testing 20 12 BGL’s (mmol/L) 4 Time
Central regulation of body weight αMSH, alpha melanocyte-stimulating hormone; AgRP, agouti-related peptide; CART, cocaine and amphetamine-regulated transcript; CCK, cholecystokinin; CRH, corticotropin-releasing hormone; GLP-1, glucagon-like peptide; MCH, melanin-concentrating hormone; NPY, neuropeptide Y; NTS, nucleus of the tractussolitarius; PP, pancreatic polypeptide; PYY, peptide YY Proietto MJA 2011;195:144–6
Diet and behavioural intervention 5 0 –5 Weight change (kg) –10 Very-low-calorie diet Modified diet plus behaviour therapy –15 Very-low-calorie diet plusbehaviour therapy –20 0 1 2 3 4 5 Intervention Years after intervention Wadden et al. Int J Obes 1989;13 Suppl 2:39–46
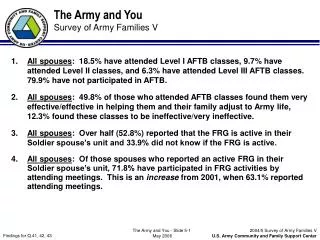
3,689,509 Patients with diabetes Unknown Number of pharmacists working in diabetes 1400+833 Nurses and doctors working in diabetes Diabetes UK. State of the Nation 2016 (England): Time to take control of diabetes. July 2016 British Medical Association. Survey of GPs in England. Nov 2016 Diabetes UK. Diabetes specialist nursing workforce survey. 2016
Current Diabetes Workforce • 84% of GPs find their workload unmanageable • 78% of Diabetes Specialist Nurses (DSNs) are concerned that their workload is having an impact on patient care and/or safety • Can pharmacists help this situation? British Medical Association. Survey of GPs in England. Nov 2016 Diabetes UK. Diabetes specialist nursing workforce survey. 2016
UK Pharmacy and Diabetes Strategy • Pharmacy and diabetes workforce policy document in development • Royal Pharmaceutical Society (RPS), NHS England and key pharmacist leaders • Context: • GP workload • Diabetes specialist nurse numbers • Diabetes specialist medical consultants • Diabetes patient numbers • Diabetes patient complexity
Diabetes Competence Framework • Access via www.diabetes.org.uk (professional competencies) • Key tool to planning your specialist portfolio • Demonstrate competencies • Action plan areas for development
RPS Professional Development Roadmap Experience in diabetes NOT career in total Royal Pharmaceutical Society. Professional development roadmap. 2016
Community Pharmacists • Front line professionals • Accessible 7 days a week, up to 24 hours a day • Advice and practical help for short-term and long-term conditions • Clinical roles: monitoring of long term conditions, medicines use reviews, new medicines service • Essential in public health promotion; risk assessments, smoking cessation, diet and exercise, sexual health
Examples: Primary Care • Cornwall and Isles of Scilly LPC: Patient Activation Measures and motivational interviewing to improve self-management of T2DM • County Durham and Darlington LPC: Just Beat It! Is a support programme to help reduce diabetes risk through education and physical activity sessions • Essex LPC: Supporting changes to blood glucose meter supplies and providing free replacement meters • Hampshire and Isle of Wight: Opportunistic identification of patients and brief intervention on footcare. Deliver simple educational messages and advice on self-care and raise awareness of deterioration • Hertfordshire LPC – Community Pharmacy Diabetes Plus: education provided to pharmacists to support patients with information “top up’s” early in diagnosis Pharmaceutical Services Negotiating Committee. Services database. September 2018.
GP practice pharmacists • London AT Medics: • 8 care processes achieved on 86% of patients • Triple target reached by 47% • Variation reduced from 82% to 30% across the practices • Devon SOAR medical: • Low spend and poor outcomes • Project to standardize approach by practice based pharmacists across 12 GP practices
Peri-operative optimization • Education of ward based pharmacists • Review of high risk pescribing • Adequate, timely medication history taking • Alerts to pharmacist to review patient • Improve access to self administration
Consultant Pharmacist Job Plan • 10 sessions (half a day) • 6 clinical (was 5 but short on medical staff currently) • 2 education and training • 1 strategy and leadership • 1 research • Rotation of clinical activity on consultant Rota • Ward rounds/ Foot clinic / Vascular MDT / Insulin Pump Clinic / Complex Diabetes Clinic / Post Discharge Clinic / Young persons Diabetes Clinic / Concentrated insulin clinic / Endocrine clinic / Lipid Clinic + referrals for paediatric type 2 diabetes
Internal Assurance of Autonomous working • 3 monthly peer review of 3 cases for whole team • 360 degree feedback from colleagues every 3 years for revalidation • 10 patient anonymous questionnaires yearly • Annual Clinical Consultant Appraisal as well as professional appraisal • Usual Continuing Professional Development (CPD)
In summary Well placed Pharmacists are present to help at every stage of the diabetes story Evidence Emerging evidences changes the choice before guidelines can be updated. Skills We know how to balance efficacy, safety, monitoring and disease management Cost Newer medicines or mechanisms of glucose testing may be more expensive, but could achieve more in the long run Knowledge Understand medicines optimisation and treatment individualisation and how to use these to empower patients Choices We have the opportunity to advise and influence treatment choices and support patients to voice their opinion