Download
1 / 1
20 likes | 236 Vues
Tibiocalcaneal Fusion using a Peg-in-Hole Technique with Combined Ilizarov External Fixation Method. Edgardo Rodriguez, DPM Byron Hutchinson, DPM Eric Powell, DPM. www.clesf.or g.

E N D
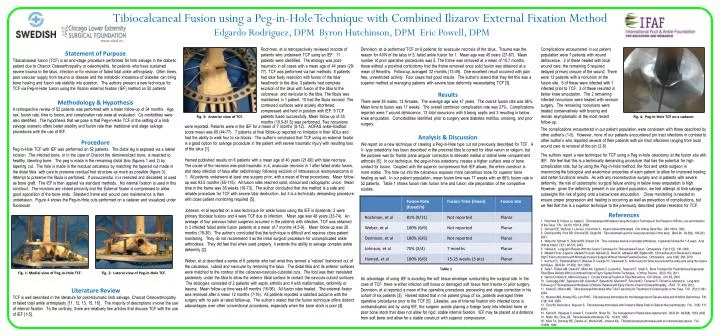
Tibiocalcaneal Fusion using a Peg-in-Hole Technique with Combined Ilizarov External Fixation Method Edgardo Rodriguez, DPM Byron Hutchinson, DPM Eric Powell, DPM www.clesf.org Rochman, et al retrospectively reviewed records of patients who underwent TCF using an IEF. 11 patients were identified. The etiology was post-traumatic in all cases with a mean age of 44 years (29-77). TCF was performed via two methods: 8 patients had talar body resection with fusion of the talar head/neck to the tibia; 3 patients had complete excision of the talus with fusion of the tibia to the calcaneus and navicular to the tibia. The fibula was maintained in 1 patient, 10 had the fibula excised. The contoured surfaces were acutely shortened, compressed and held in position with IEF. 9 TCF patients fused successfully. Mean follow-up of 35 months (10.5-81.5) was performed. Two nonunions Dennison, et al performed TCF on 6 patients for avascular necrosis of the talus. Trauma was the reason for AVN of the talus in 5, failed ankle fusion for 1. Mean age was 45 years (27-67). Mean number of prior operative procedures was 5. The frame was removed at a mean of 10.7 months, those without a proximal corticotomy had the frame removed once solid fusion was obtained at a mean of 9months. Follow-up averaged 32 months (13-49). One excellent result occurred with pain free, unrestricted activity. Four cases had good results. The author’s stated that they felt this was a superior method at managing patients with severe talar deformity necessitating TCF [3]. Complications encountered in our patient population were 7 patients with wound dehiscence. 2 of these healed with local wound care; the remaining 5 required delayed primary closure of the wound. There were 13 patients with a nonunion at the fusion site. 5 of these were infected with 1 infected prior to TCF. 3 of these resulted in below knee amputation. The 2 remaining infected nonunions were treated with revision surgery. The remaining nonunions were treated conservatively with bracing and remain asymptomatic at the most recent follow-up. Statement of Purpose • Tibocalcaneal fusion(TCF) is an end-stage procedure performed for limb salvage in the diabetic patient due to Charcot Osteoarthropathy or osteomyelitis, for patients who have sustained severe trauma to the talus, infection or for revision of failed total ankle arthroplasty. Often times, poor vascular supply from trauma or disease and the metabolic imbalance of diabetes can bring bone healing and fusion site stability into question. Theauthors present a new technique for TCF via Peg-in-Hole fusion using the Ilizarov external fixation (IEF) method on 52 patients Results There were 39 males, 13 females. The average age was 47 years. The overall fusion rate was 86%. Mean time to fusion was 17 weeks. The overall combined complication rate was 27%. Complications reported were 7 wound dehiscence, 13 total nonunions with 5 being septic and 3 resulting in below knee amputation. Comorbidities identified prior to surgery were diabetes mellitus, smoking, and prior surgery. Methodology & Hypothesis A retrospective review of 52 patients was performed with a mean follow-up of 34 months. Age, sex, fusion rate, time to fusion, and complication rate were all evaluated. Co-morbidities were also identified. The hypothesis that we pose is that Peg-in-Hole TCF in the setting of a limb salvage scenario offers better stability and fusion rate than traditional end stage salvage procedures with the use of IEF. Fig. 3: Anterior view of TCF. Fig. 4: Peg-in-Hole TCF on a cadaver. were reported. Patients were in the IEF for a mean of 7 months (5-12). AOFAS ankle-hindfoot score mean was 65 (44-77). 7 patients at final follow-up reported no limitation in their ADLs and had the ability to walk four to six blocks. The author’s concluded that TCF using an external fixator is a good option for salvage procedure in the patient with severe traumatic injury with resulting loss of the talus [1]. Hamed published results on 6 patients with a mean age of 40 years (21-60) with talar necrosis. The cause of the necrosis was post-traumatic in 4, avascular necrosis in 1 after failed ankle fusion, and deep infection of talus after radiotherapy following excision of intraosseousleiomyosarcoma in 1. All patients underwent at least one surgery prior, with a mean of three procedures. Mean follow-up was 93.5 months (55-115). All fusion sites reached solid, clinical and radiographic union. Mean time in the frame was 36 weeks (16-73). The author concluded that this method is a safe and reliable procedure for TCF with severe talar destruction, but it is a technically demanding procedure with close patient monitoring required [5]. Johnson, et al reported on a new technique for ankle fusion using the IEF in 6patients; 2 were primary tibiotalar fusions and 4 were TCF due to infection. Mean age was 48 years (33-74). An average of four previous failed surgeries occurred in the patients with infection. TCF was obtained in 3 infected failed ankle fusion patients at a mean of 7 months (4.5-9). Mean follow-up was 26 months (19-30). The author’s concluded that the technique is difficult and requires close patient monitoring. They do not recommend it as the initial surgical procedure for uncomplicated ankle arthrodesis. They did feel that when used properly, it extends the ability to salvage complex ankle deformity [2]. Weber, et al described a series of 6 patients who had what they termed a “rabbet” fashioned out of the calcaneus, cuboid and navicular by removing the talus. The distal tibia and its anterior surfaces were matched to the contour of the calcaneo-naviculo-cuboidal cuts. The foot was then translated posteriorly under the tibia to allow the anterior tibial surface to contact the naviculo-cuboid surfaces. The etiologies consisted of 2 patients with septic arthritis and 4 with malformation, deformity or trauma. Mean follow-up time was 46 months (16-96). All fusion sites healed. The external fixator was removed after a mean 12 months (7-16). All patients reported a satisfied outcome with the surgery with no pain at latest follow-up. The author’s stated that the fusion technique offers distinct adavantages over other conventional procedures, especially when the bone stock is poor [4]. The complications encountered in our patient population were consistent with those described by other author’s (1-5). However, none of our patients encountered pin tract infections in contrast to other author’s who reported several of their patients with pin tract infections ranging from local wound care to removal of the pin (2-5) Analysis & Discussion We report on a new technique of creating a Peg-in-Hole type cut not previously described for TCF. A V- type osteotomy has been described in the proximal tibia to correct for tibialvarumor valgum, but the purpose was for frontal plane angular correction to alleviate medial or lateral knee compartment arthrosis [6]. In our technique, the peg-in-hole osteotomy creates a higher surface area of bone contact for fusion. Coupled with the superior compression that IEF allows, the entire construct is more stable. The hole cut into the calcaneus exposes more cancellousbone for superior bone healing as well. In our patient population, mean fusion time was 17 weeks with an 86% fusion rate in 52 patients. Table 1 shows fusion rate, fusion time and fusion site preparation of the compartive studies.. An advantage of using IEF is avoiding the soft tissue envelope surrounding the surgical site. In the case of TCF, there is either infected soft tissue or damaged soft tissue from trauma or prior surgery. Dennison, et al reported a mean of five operative procedures proceeding end stage correction in his cohort of six patients [3]. Hamed stated that in his patient group of six, patients averaged three operative procedures prior to the TCF [5]. Likewise, use of internal fixation into infected bone is contraindicated and by using IEF, the surgeon avoids placing a foreign body into infected bone or poor bone stock that does not allow for rigid, stable internal fixation. IEF may be placed at a distance from soft bone and allow for a stable construct with superior compression. Procedure Peg-in-Hole TCF with IEF was performed on 52 patients. The distal leg is exposed via a lateral incision. The infected bone, or in the case of Charcot the demineralized bone, is resected to healthy, bleeding bone. The peg is made in the remaining distal tibia (figures 1 and 2) by tapering cut. The hole is made in the residual calcaneusby matching the tapered cut made in the distal tibia with care to preserve residual foot structure as much as possible (figure 3). Attempt to preserve the fibula is perfomed. If unsuccessful, it is resected and discarded or used as bone graft. The IEF is then applied via standard methods. No internal fixation is used in this construct. The incisions are closed primarily and the External fixator is compressed to allow good apposition of the bone ends. Standard frame and wound care maintenance is then undertaken. Figure 4 shows the Peg-in-Hole cuts performed on a cadaver and visualized under fluoroscan The authors report a new technique for TCF using a Peg-in-hole osteotomy at the fusion site with IEF. We feel that this is a technically demanding procedure that has the potential for high complication rate, but by using the Peg-in-Hole method, the foot and ankle surgeon is maximizing the biological and anatomical properties of each patient to allow for improved healing and better functional results. As with any reconstructive surgery and in patients with severe deformity, the risk of catastrophic surgical failure ending in below knee amputation is high. However, given the deformity present in our patient population, we feel attempt at limb salvage outweighs the risk of going onto a below knee amputation. Close monitoring is needed to ensure proper progression and healing is occurring as well as prevention of complications, but we feel that this is a superior technique to the previously described planar resection for TCF. References 1. Rochman R, Hutson JJ, Alade O. TibiocalcanealArthrodesis Using the Ilizarov Technique in the Presence of Bone Loss and Infection of the Talus. FAI. 29(10): 1001-8, 2008. 2. Johnson EE, Weltmer J, Lian GJ, Cracchiolo A. Ilizarov Ankle Arthrodesis. ClinOrthopRelat Res. 280: 160-9, 1992. 3. Dennison MG, Pool RD, Simonis RB, Singh BS. Tibiocalcaneal fusion for avascular necrosis of the talus. JBJS-Br. 83-B(2): 199-203, 2001. 4. Weber M, Schwer H, Zilkens KW, Siebert CH. Tibio-calcaneo-naviculo-cuboidalearthrodesis: 6 patients followed for 1-8 years. ActaOrthop Scand 73(1): 98-103, 2002. 5. Hamed K. Long-term Results With the Ilizarov Technique for Tibiocalcaneal Fusion. Orthopedics. Feb 31(2): 130, 2008. 6. MadadiFirooz, Eajazi A, MadadiFiroozeh, Behseli LD, Rokni R, Abbasian MR, Bigdeli MR. Clinical Results of Reversed V-shaped High TibialCorticotomy with Minimally Invasive Surgery Without Internal Fixation Devices. Orthopedics. June 33(6): 388, 2010. 7. KoVoor CC, Padmanabham V, Bhaskar D, George VV, Viswanath S. Ankle fusion for bone loss around the ankle joint using the Ilizarov technique. JBJS-Br. 91-B(3): 361, 2009. 8. Sala F, Thabet AM, Castelli F, Miller AN, Capitani D, Lovisetti G, Talamonti T, Singh S. Bone Transport for Postinfectious Segmental Tibial Bone Defects With a Combined Ilizarov/Taylor Spatial Frame Technique. J Orthop Trauma. 25(3): 162, 2011. 9. Garcia-Cimbrelo E, Marti-Gonzalez J. Circular External Fixation in TibialNonunions. ClinOrthop. 419: 65, 2004. 10. Caravaggi CMF, Sganzaroli AB, Galenda P, Balaudo M, Gherardi P, Simonetti D, Ferraresi R, Farnetti A, Morandi A. Long-term Follow-up of TibiocalcanealArthrodesis in Diabetic Patients with Early Chronic Charcot Osteoarthropathy. JFAS. 51: 408, 2012. 11. Kolker D, Wilson MG. TibiocalcanealArthrodesis After Total Talectomy for Treatment of Osteomyelitis of the Talus. FAI. 25(12): 861, 2004. 12. Myerson MS, Alvarez RG, Lam PWC. TibiocalcanealArthrodesis for the Management of Severe Ankle and Hindfoot Deformities. FAI. 21(8): 643, 2000. 13. Cinar M, Derincek A, Akpunar S. TibiocalcanealArthrodesis with Posterior Blade Plate in Diabetic Neuroarthropathy. FAI. 31(6): 511, 2010. 14. Kotnis R, Pasapula C, Anwar F, Cooke PH, Sharp RJ. The management of failed ankle replacement. JBJS-Br. 88-B(8): 1039, 2006. 15. Mann RA, Chou LB. Tibiocalcanealarthrodesis. FAI. 16:401, 1995. 16. Kilen TA, Donnelly RE, Gehrke JC, Werner ME, Johnson KA. Tibiotalocalcanealarthrodesis with an intramedullary device. FAI. 15:669, 1994. Table 1 Fig. 1: Medial view of Peg-in-Hole TCF. Fig. 2: Lateral view of Peg-in-Hole TCF. • Literature Review • TCF is well described in the literature for post-traumatic limb salvage, Charcot Osteoarthropathy or failed total ankle arthroplasty [11, 12, 13, 15, 16] . The majority of descriptions involve the use of internal fixation. To the contrary, there are relatively few articles that discuss TCF with the use of IEF [1-5].