Download
1 / 28
310 likes | 561 Vues
Disorders of the Female Reproductive Tract. Cancer. I. Cancer in Situ. A pre-invasive, asymptomatic CA Can only be diagnosed by examination of cervical cells via microscope Can be treated without radical surgery Is 100% curable. II. Management of CA in Situ. Electrocautery Cryosurgery

E N D
I. Cancer in Situ • A pre-invasive, asymptomatic CA • Can only be diagnosed by examination of cervical cells via microscope • Can be treated without radical surgery • Is 100% curable
II. Management of CA in Situ • Electrocautery • Cryosurgery • Laser • Conization • Hysterectomy
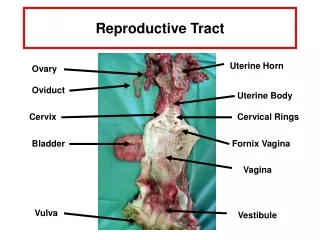
III. Cancers of the Reproductive Tract – Cervix • Those @ risk: • Sexually active as teens • Multiple births • socioeconomic levels • STDs
Cervix – etiology (con’t) • HPV (human papilloma virus) • Smoking • Whose mothers took DES • Infections & erosion of the cervix
Cervix – S/sx • Silent in early stages w/ few sx • Leukorrhea • Irregular vaginal bleeding/spotting between menses • Bleeding after coitus or after menopause • Bleeding slight @ 1st, then increases w/ progression of disease
Cervix – S/sx (con’t) • Vaginal exudate • Becomes watery • & becomes dark bloody & odiferous d/t necrosis & infection • Severe pain in back, legs & upper thighs w/ advanced stages
Cervix – Dx Tests • Pap Smear • Schiller’s test • Cervical biopsy • CT, etc as needed • Cervical screening – 3 yrs after having sex but no later than age 21 & prn
Cervix – Med Mgmt • Early CA of cervix treated with hysterectomy or intracavity radiation • Radical hysterectomy includes pelvic lymph node dissection; then chemo & radiation • Internal radiation done on in-patient status
Cervix – NI • Reassurance • Hospice care if CA well advanced • Change dressings & peri-pads often • Monitor skin integrity closely
B. Endometrium – Etiology • Usually affects post-menopausal women • Either localized or may metastasize • @ risk • Irregular periods • Menopause difficulties
Endometrium – Etiology (con’t) • @ risk (con’t) • Obesity • HTN • DM • HRT • On Tamoxifen (anti-neoplastic)
Post-menopausal bleeding (50% have CA) Report any type of abnormal bleeding, regardless of age Pelvic exam Rectal exam D&C Endometrium – S/sx Dx Tests
Endometrium – Med Mgmt • Depends on tumor stage & health status • Surgery, radiation, chemotherapy • TAH-BSO • Intracavity radiation • All tx tailored individually
Endometrium – NI • Regular exams after interventions (surgery, chemo, radiation) • Compliance with treatment plan • Primarily an adenocarcinoma & slow growing giving adequate time for appropriate intervention
C. Ovary – Etiology • Tumors asymptomatic in early stages • Has become metastatic when diagnosed • Those @ risk: • Oral contraceptives • heredity
Ovary – Etiology (con’t) • Those @ risk: • Infertile, anovulatory, nulliparous, habitual aborters • Oral contraceptive use > 5 yrs • fat diet • Industrial chemical exposure (asbestos & talc)
Vague sx: abd pain, flatulence, mild gastric c/o Abdominal girth enlarges Flatulence with distention Other sx: Frequency, N/V, constipation, wt loss Ovary – S/sxEarly stage Later stage
Ovary – Dx Tests • Bi-manual exam • CT of the pelvis • Tumor bx • Exploratory laparoscopy • CA-125 Is it a positive test? • Aspiration of ascitic fluid
Ovary – Med Mgmt • TAH-BSO & omentectomy (excision of part of peritoneal folds) • Chemo • Radiation
Ovary – NI • Same as w/ TAH-BSO, radiation & chemo • All for venting/verbalizing • Possibly palliative care
IV. Epidemiology of Ovarian CA • Risk increases with age • Peaks in late 70’s • Hereditary accounts for 5% - 10% of all ovarian CA • 2004: of 25,580 diagnosed, 16,090 would die 63%
V. Therapies for CA • Surgery • Radiation therapy • Internal • External • chemotherapy
VI. Hysterectomy – Vaginal • Done more often than abd approach • No incision • Lithotomy position • Shorter in-hospital stay • Fewer complications • 10 yrs after surgery stress incontinence may occur
Hysterectomy – Abdominal • Sub-total: removes only midsection of the uterus • Total: removes uterus & cervix, leaving tubes & ovaries • TAH-BSO: removes everything • What is concern with a sub-total?
Hysterectomy – Abdominal Pre-op • Low residue diet • Fleets enema @ HS • Antiseptic vaginal douche (betadine)
VII. Post-op NI for Hysterectomy • Monitoring VS • Preventing UA retention, intestinal distention & venous thrombosis • Early ambulating • Harris flush, prn • TEDS or SCDs • Pain control, often w/ PCA
Post-op NI for Hysterectomy (con’t) • No sex X 4-6 weeks post-op • No heavy lifting, long car rides • Vaginal discharge X 2-4 weeks • Report any s/sx of infection • Malodorous vaginal exudate • Hyperthermic @ 101 F • S/sx of UTI