Download
1 / 82
820 likes | 1.04k Vues
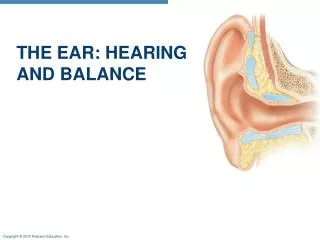
Ear and Hearing Problems Disorders. Dr Ibraheem Bashayreh, RN, PhD. Anatomy of the Ear. External Otitis. Painful condition caused when irritating or infective agents come into contact with the skin of the external ear Commonly called swimmer’s ear

E N D
Ear and Hearing Problems Disorders Dr Ibraheem Bashayreh, RN, PhD
External Otitis Painful condition caused when irritating or infective agents come into contact with the skin of the external ear Commonly called swimmer’s ear Two most common precipitants are excessive mositure and trauma to ear canal. 2 most common presenting symptoms are “otalgia” (ear discomfort) and “otorrhea” (discharge from external ear canal). Common symptoms are pain, itching, tenderness, and temporary loss of hearing.
External Otitis Treatment focused on reducing inflammation, edema, and pain with heat, bedrest, limited head movement, topical antibiotic and steroid therapy, and analgesics
Furuncle Localized external otitis caused by bacterial infection of a hair follicle Hearing impaired if the lesion blocks the canal, most commonly cerumen (wax) Treatment with local and systemic antibiotics, heat application, earwick to relieve pain, and possible incision and drainage
Cerumen or Foreign Bodies Cerumen (wax) is the most common cause of an impacted canal. Function Lubrication, Trapping, Waterproof barrier, Antimicrobial, Inhibitory pH Other blockages include vegetables, beads, pencil erasers, insects.
Ear Wax Content Appearance Color
Treatment Rx: Irrigate canal with a mixture of water and hydrogen peroxide at body temperature for impacted cerumen; Cerumenex softens wax. Carefully remove foreign object.
Water-clogged ear Not the same as Swimmer’s Ear (Otitis externa) Some people are more prone to retaining water Signs and symptoms include feeling of fullness, wetness, gradual hearing loss, itching, pain, inflammation, or infection. So can end up with otitis externa.
Treatment Tilting the effected ear Use of blow dryer Isopropyl alcohol 95% in anhydrous glycerin 5% 50:50 mixture of acetic acid 5% (white vinegar) and isopropyl alcohol 95%
Otitis Media * One of the most common childhood illnesses. * Approximately $3 billion in healthcare costs were attributed to >5 million cases in 1995 Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old.
Otitis Media Three types of otitis media include: Acute otitis media Chronic otitis media Serous otitis media Most commonly reported symptoms are cough, rhinitis, fever, and earache.
Nonsurgical Management Quiet environment Bedrest with limited head movement Heat and cold applications Systemic and topical antibiotic therapy Analgesics Antihistamines Decongestants
Surgical Management Myringotomy is a surgical opening of the pars tensa of the eardrum. Operative procedure includes grommet (polyethylene tube) placed through the tympanic membrane. Postoperative care: keep external ear and canal free of other substances while the incision is healing and keep head dry for several days.
Mastoiditis Infection of the mastoid air cells caused by untreated or inadequately treated otitis media Nonsurgical management: antibiotics (Continued)
Mastoiditis (Continued) Surgical management: simple or modified radical mastoidectomy with tympanoplasty Complications: damage to cranial nerves, vertigo, meningitis, brain abscess, chronic purulent otitis media, and wound infection
Trauma Trauma and damage to the eardrum and ossicles may occur by infection, by direct damage, or through rapid changes in the middle-ear cavity pressure. Eardrum perforations usually heal within 24 hours. Use preventive measures to protect the ear from trauma.
Neoplasms Tumors are removed by surgery, which often destroys hearing in affected ear. Benign lesions are removed because, with continued growth of the neoplasm, other structures can be affected, damaging the facial or trigeminal nerve. When possible, reconstruction of the middle ear structures is performed.
Tinnitus Continuous ringing or noise perception is one of the most common problems with ear or hearing disorders. Tinnitis cannot be observed or confirmed with diagnostic tests. When no cause is found, therapy focuses on masking the tinnitus with background sound, noisemakers, and music during sleeping hours.
Vertigo and Dizziness Common manifestations of many ear disorders Advise client to: Restrict head motions and move more slowly. Maintain adequate hydration. Take antivertiginous drugs. Prevent loss-of-balance accidents.
Labyrinthitis Infection of the labyrinth Meningitis a common complication of labyrinthitis Treatment with systemic antibiotics, bedrest in a darkened room, antiemetics, antivertiginous medications, psychosocial support
Meniere’s Disease Affects 200/100,000 people Inner chronic ear Disorder A typical Acute Attack causes vertigo, tinnitus, feeling of fullness and pressure in ear, fluctuating hearing loss, nausea and vomiting. Average acute attack lasts 2-4 hours and leaves patient exhausted. Patient tends to sleep for hours after acute attacks Is there a Cure??
Ménière's Disease Rx Nonsurgical management includes slow head movements, salt and fluid restrictions, cessation of smoking, mild diuretics, nicotinic acid, antihistamines, antiemetics, diazepam. Surgical management is a last resort and consists of labyrinthectomy (Excision of the labyrinth of the ear) or endolymphatic decompression with drainage and shunt. Hearing in the affected ear is often sacrificed.
Acoustic Neuroma Benign tumor of eighth cranial nerve Surgical removal via craniotomy Extreme care taken to preserve the function of the facial nerve
Hearing Loss One of the most common physical handicaps in North America. Common causes of conductive hearing loss: any inflammation process or obstruction of the external or middle ear by cerumen or foreign objects. (Continued)
Hearing Loss(Continued) Common causes of sensorineural hearing loss: loud noise, drugs, atherosclerosis, hypertension, prolonged fever, Ménière's disease, diabetes mellitus, and ear surgery.
Assessments Tuning fork tests Otoscopic examination Psychosocial assessment Laboratory tests Radiographic assessment Other diagnostic assessments such as audiogram
Treatment of Hearing Loss Drug therapy Assistive devices Hearing aids Cochlear implants (Continued)
Treatment of Hearing Loss(Continued) Tympanoplasty Postoperative care includes antiseptic-soaked gauze packed in the ear canal, clean dressing, client flat with head turned to the side and the operative ear facing up for at least 12 hours after surgery, prescribed antibiotics, activity restrictions.
Stapedectomy A partial or complete stapedectomy with a prosthesis corrects hearing loss and is most effective for hearing loss related to otosclerosis. Hearing improvement may not occur until 6 weeks after surgery. (Continued)
Stapedectomy (Continued) Damage to cranial nerves, vertigo, and nausea and vomiting are common after surgery. Pain medications and antibiotics are often used. Safety measures and antivertiginous drugs should be applied.
Epistaxsis • Precipitating factors • Trauma • Picking • Blunt contact • Drying of nasal mucous membranes • Infection • Substance abuse • Arteriosclerosis • Hypertension • Bleeding disorders • Anticoagulant therapy
Epistaxsis • Clinical Manifestations • 90% anterior nasal septum • Trauma • Drying • Infection • Posterior secondary to • Blood dyscrasias • Hypertension • Diabetes • Tends to be more severe • Occurs more frequently in older adult
Epistaxsis • Management • Anterior • Simple first aid • Apply pressure for 5-10 minutes • Apply ice packs to nose & forehead • Sitting position leaning forward • Discourage swallowing blood • Medications • Topical vasoconstrictors • Cocaine • Neo-Synephrine • Adrenaline • Nasal spray or on cotton swab held against bleeding site
Epistaxsis • Medications cont’d • Chemical cauterization • Silver nitrate • Gelfoam • Topical anesthetic (pre packing) • Tetracaine • Lidocaine • Cocaine • Nasal Packing ~ Anterior • Petroleum gauze • 24-72 hours commonly
Epistaxsis • Nasal Packing ~ Posterior • Pack both anterior & posterior • 2-5 days
Epistaxsis • Posterior Packing cont’d • Monitor for hypoxemia • Administer oxygen as ordered • Frequent oral hygiene • Administer narcotic analgesics as ordered • Monitor for complications • Toxic shock syndrome • Otitis media • Sinusitis
Epistaxsis • Endoscopic Surgery • Cauterizing bleeding vessel • Ligation of internal maxillary artery
Nasal Polyps • Benign grapelike growth of mucous membrane
Nasal Polyps • Form in areas of dependent mucous membrane • Usually bilateral • Stem-like base makes them moveable • May enlarge nasal obstruction
Nasal Polyps • Management • Topical corticosteroid nasal spray • Low-dose oral corticosteroids • Surgery • Polypectomy under local anesthesia • Nasal packing to control bleeding • Avoid blowing nose 24-48 hours post removal of packing • Avoid straining at stool, vigorous coughing, strenuous exercise • Monitor for bleeding • Frequent swallowing • Visible blood at back of throat • Laser surgery to remove polyps • May require multiple surgeries as polyps tend to recur
Deviated Septum • May result from trauma • Causes nasal obstruction
Deviated Septum • Surgery • Septoplasty or submucous resection • Manipulation of septal cartilage • Post operatively • Bilateral nasal packing
Rhinoplasty • Surgical reconstruction of the nose • Relief of airway obstruction • Repair visible deformity • Reshaping of nose by • Moving • Rearranging • Augmenting
Rhinoplasty • Post operatively • Nasal packing for 72 hours • Temporary plastic splint for 3-5 days • Swelling subsides within 10-14 days • Normal sensation returns within several months
Sinusitis • Inflammation of mucous membranes of sinuses • Acute or chronic • Follows upper respiratory infection • Organisms • Streptococci • Streptococcus pneumoniae • Haemophilus influenzae • Staphylococci