Download
1 / 48
480 likes | 483 Vues
This article discusses the different types and classification of pneumonia, including lobar pneumonia, interstitial pneumonia, and broncho pneumonia. It also explores the various causes and complications of pneumonia, such as bacterial invasion, aspiration, and chronic pneumonia. Additionally, it emphasizes the importance of identifying the causative agent and extent of the disease for effective treatment.

E N D
Defence lost! • Loss or suppression of the cough reflex, coma, anesthesia, neuromuscular disorders, drugs, • Injury to the mucociliary apparatus, • impairment of ciliary function or • destruction of ciliated epithelium - cigarette smoke, inhalation of hot or corrosive gases, viral diseases, or genetic defects of ciliary function (e.g., the immotile cilia syndrome)
Accumulation of secretions cystic fibrosis, bronchial obstruction • Interference with the phagocytic or bactericidal action of alveolar macrophages alcohol, tobacco smoke, anoxia, or oxygen intoxication • Pulmonary congestion and edema
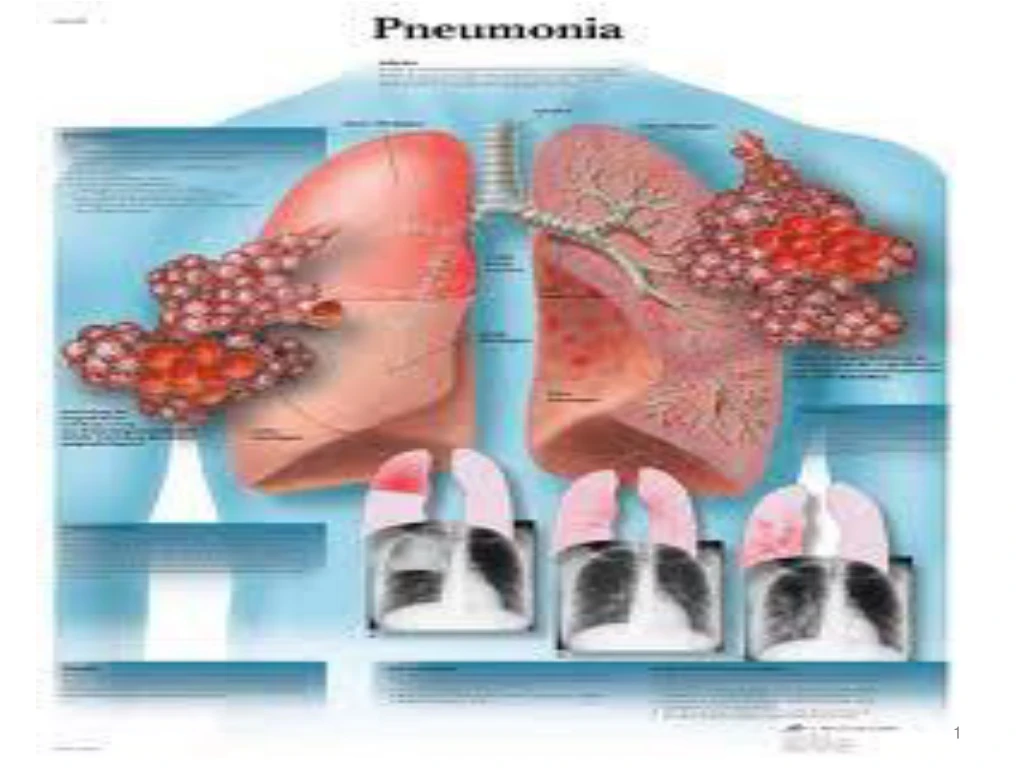
PNEUMONIA • Pneumonia is the inflammation of the pulmonary parenchyma . • Clinically pneumonia may occur either as a primary disease or as a complication of another illness.
Bacterial invasion of the lung parenchyma causes the alveoli to be filled with an inflammatory exudate, causing consolidation (“solidification”) of the pulmonary tissue.
TYPES • LOBAR PNEUMONIA: • INTERSTITIAL PNEUMONIA • BRONCHO PNEUMONIA
CLASSIFICATION • Viral • Bacterial • Mycoplasmal • Aspiration of foreign substances • Bacterial
Pneumonia syndromesclinical setting & etiological agent • Community-acquired acute pneumonia • Community-acquired atypical pneumonia • Hospital-acquired pneumonia • Aspiration pneumonia • Chronic pneumonia • Necrotizing pneumonia & lung abscess • Pneumonia in the immunocompromised host
COMMUNITY-ACQUIRED ACUTE PNEUMONIA • Streptococcus pneumoniae • Haemophilusinfluenzae • Moraxella catarrhalis • Staphylococcus aureus • Legionella pneumophila • Enterobacteriaceae (Klebsiellapneumoniae) • Pseudomonas
COMMUNITY-ACQUIRED ATYPICAL PNEUMONIA • Mycoplasma pneumoniae • Chlamydia (C. pneumoniae, C. psittaci, C trachomatis) • Coxiellaburnetii (Q fever) • Viruses: respiratory syncytial virus, parainfluenza virus (children); influenza A and B (adults); adenovirus (military recruits); SARS virus (severe acute respiratory syndrome)
HOSPITAL-ACQUIRED PNEUMONIA Gram-negative rods, Enterobacteriaceae (Klebsiella, Serratia marcescens, Escherichia coli) Pseudomonas Staphylococcus aureus (usually penicillin resistant)
ASPIRATION PNEUMONIA • Anaerobic oral flora (Bacteroides, Prevotella, Fusobacterium, Peptostreptococcus), admixed with aerobic bacteria (Streptococcus pneumoniae, Staphylococcus aureus, Haemophilusinfluenzae, Pseudomonas aeruginosa)
CHRONIC PNEUMONIA • Nocardia • Actinomyces • Granulomatous: Mycobacterium tuberculosis, atypical mycobacteria, Fungi Histoplasmacapsulatum, Coccidioidesimmitis, Blastomycesdermatitidis
NECROTIZING PNEUMONIA & LUNG ABSCESS • Anaerobic bacteria (extremely common), with or without mixed aerobic infection • Staphylococcus aureus, • Klebsiellapneumoniae, • Streptococcus pyogenes, • pneumococcus (uncommon)
PNEUMONIA IN THE IMMUNOCOMPROMISED HOST • Cytomegalovirus • Pneumocystis jiroveci • Mycobacterium avium-intracellulare • Invasive aspergillosis • Invasive candidiasis • “Usual” bacterial, viral, and fungal organisms • (listed above)
Predisposing factors • extremes of age, • chronic diseases (congestive heart failure, COPD, diabetes), • congenital or acquired immune deficiencies, • decreased or absent splenic function (sickle cell disease or post-splenectomy,
Bacterial pneumonia has two patterns of anatomic distribution: bronchopneumonia lobar pneumonia Patchy consolidation of the lung is the dominant characteristic of bronchopneumonia fibrinosuppurative consolidation of a large portion of a lobe or of an entire lobe defines lobar pneumonia
Bronchopneumonia • Patchy consolidation of the lung
Lobar pneumonia • consolidation of a large portion of a lobe or of an entire lobe
Most important from the clinical standpoint are identification of the causative agent and determination of the extent of disease.
In lobar pneumonia, four stages of the inflammatory response have classically been described: • Congestion, • Red hepatization, • Grey hepatization, • Resolution
Congestion • “Vascular event” • Gross: the lung is heavy, boggy, and red. Microscopy: vascular engorgement – congested septal capillaries intra-alveolar fluid with only few neutrophils, often the presence of numerous bacteria.
Red hepatization • Microscopy: massive confluent exudation with neutrophils, red cells, and fibrin filling the alveolar spaces • On gross examination, the lobe now appears distinctly red, firm, and airless, with a liver-like consistency, hence the term hepatization.
Grey hepatization • progressive disintegration of red cells and the persistence of a fibrinosuppurative exudate • Few neutrophils, many macrophages, retraction of the exudate • giving the gross appearance of a grayish brown, dry surface
Resolution • the consolidated exudate within the alveolar spaces undergoes progressive enzymatic digestion • to produce granular, semifluid debris • that is resorbed / ingested by macrophages / expectorated / organized by fibroblasts growing into it resolved!
Clinical manifestation • Child appears ill, drowsy • Fever with chills • Malaise • Rapid and shallow respiration • Cough • Chest pain
PneumoniaDiagnosis • History taking • Physical examination • Chest x-ray • Blood routine • Sputum culture
Complications • (1) Pleural fibrinous reaction to the underlying inflammation, often present in the early stages if the consolidation extends to the surface (pleuritis) • may resolve • pleural effusion • More often it undergoes organization, leaving fibrous thickening or permanent adhesions.
(2) spread of infection to the pleural cavity, causing the intrapleural fibrinosuppurative reaction known as empyema • or Pyopneumothorax
(3) tissue destruction and necrosis, causing abscess formation
(4) bacteremic dissemination to the heart valves, pericardium, brain, kidneys, spleen, or joints, causing metastatic abscesses, endocarditis, meningitis, or suppurative arthritis.
prognosis • Prognosis is generally good with rapid recovery when symptoms are recognized and treated early • Steptococcal infection – resolve spontaneously • Staphylococcal pneumonia- prolonged.
LUNG ABSCESS • Aspiration of infective material (the most frequent cause): acute alcoholism, coma, anesthesia, sinusitis, gingivodental sepsis, and debilitation • the cough reflexes are depressed. • Antecedent primary lung infection: Post-pneumonic S. aureus, K. pneumoniae, pneumococcus. • Posttransplant or otherwise immunosuppressed individuals are at special risk.
LUNG ABSCESS • Antecedent primary lung infection: • Post-pneumonic - S. aureus, K. pneumoniae, pneumococcus. • Posttransplant or otherwise immunosuppressed individuals are at special risk.
LUNG ABSCESS • Septic embolism: • Infected emboli from thrombophlebitis in any portion of the systemic venous circulation • or from the vegetations of infective bacterial endocarditis on the right side of the heart are trapped in the lung
LUNG ABSCESS • Neoplasia: Secondary infection is particularly common in the bronchopulmonary segment obstructed by a primary or secondary malignancy (postobstructive pneumonia).
LUNG ABSCESS • Miscellaneous: • Direct traumatic penetrations of the lungs; • spread of infections from a neighboring organ, such as suppuration in the esophagus, spine, subphrenic space, or pleural cavity; • and hematogenous seeding of the lung by pyogenic organisms


















