Download
1 / 28
331 likes | 1.83k Vues
Abnormal composition of urine. mirka.rovenska@lfmotol.cuni.cz. Urine examination. Physical – volume, density, colour, odour, turbidity Chemical Examination of urine sediment. Routine: pH proteins ketone bodies glucose blood in the urine nitrite s leukocytes . T argeted:

E N D
Abnormal composition of urine mirka.rovenska@lfmotol.cuni.cz
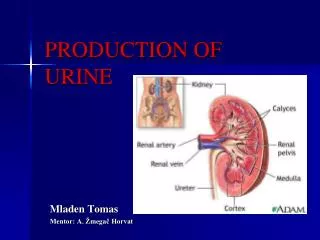
Urine examination • Physical – volume, density, colour, odour, turbidity • Chemical • Examination of urine sediment
Routine: pH proteins ketone bodies glucose blood in the urine nitrites leukocytes Targeted: bilirubin, urobilinogen amino acid metabolites hormones (cortisol, sex hormones, somatotropin) Chemical examination of urine
pH of urine • Usual range: 5,5 – 7,0 (maximal range: 4,5 – 7,5) • Aciduria – pH < 5,4 • Cause: • diet high in meat products (sulphur and phosphorus are metabolized to sulphates and phosphates) • compensation of metabolic / respiratory acidosis • along with ketonuria can be predictive of starving/lack of saccha-rides; if glucosuria is also present, the combination can indicate decompensated DM • Alkaluria (alkalinuria) – pH > 6,5 • Cause: • lacto vegetarian diet • urinary tract infection (bacterial urease) • compensation of respiratory / metabolic alkalosis at its onset
Proteins in urine • Proteinuria = excessive excretion of proteins into the urine: >150 mg/d • Cause: • physiological: physical effort • pathological: • renal disease – according to the origin: • glomerular proteinuria • tubular proteinuria • glomerular and tubular proteinuria • post-renal proteinuria –either bleeding into the urinary tract, or local secretion of immunoglobulin • pre-renal proteinuria – due to an increased plasma concentration of low-molecular proteins ( increased excretion into the urine)
Ketone bodies • Acetone, acetoacetate, -hydroxybutyrate • Synthesis: from acetyl-CoA, produced by -oxidation of fatty acids • Starvation, physical effort, stress lipolysis and -oxidation of FA; acetyl-CoA is used preferentially for the synthesis of ketone bodies
Ketonuria • level of ketone bodies in the urine (normally – very low) • Causes: • severe DM • long-term starvation, marked reduction of saccharides in diet • tenacious vomiting • Test strips: acetoacetate (not -HB!) reacts with nitroprusside (in the presence of alkali), producing purple-coloured complexes (Legal reaction)
Glucose in urine • Physiological range: 0,1 – 1,4 mmol/l • Test strips: glucose is oxidized by glucose oxidase; H2O2 is formed that converts a colourless substrate to a coloured complex • Glucosuria (glycosuria) = increased amount of glucose in the urine; causes: • hyperglycaemia > 10 mmol/l (DM, acute pancreatitis…) • renal glycosuria (glucose is abnormally excreted by the kidney) • increased intestinal reabsorption
Blood in urine • A) hematuria (erythrocyturia) – causes: • renal disease (glomerulonephritis, tumours) • other diseases of the urinary tract • haemorrhagic diathesis (e.g. thrombocytopathy,haemophilia) • B) hemoglobinuria – excessive intravascular haemolysis (haemolytic anaemia, e.g. hereditary or after non-compatible transfusion) • Test: • i)test strip detecting hemoglobin:Hb catalyzes oxidation of the substrate with peroxide to a coloured product (pseudoperoxidase activity) • ii) erythrocytes in the urinary sediment
Nitrites in urine • Nitrates in the urine can by reduced by some pathogenic bacteria to nitrites that can thus serve as indicators of the infection in the urinary tract • These bacteria include: E. Coli, Klebsiella, Salmonella, Proteus, Aerobacter, Citrobacter, some strains of Enterococcus, Staphylococcus, Pseudomonas
Leukocytes in urine • Increased amount of leukocytes (> 20/µl) – pyuria – is a sign of inflammation in the urinary tract • Test: granulocyte esterase activity • Causes: • infection of the urinary tract • tumours
heme→ biliverdin → bilirubin transport to the liver (albumin) conjugation with glucuronate bilirubin diglucuronide secreted into the bile bacteria in the small intestine release bilirubin from diglucuronide and convert it to colourless urobilinogens a small fraction is reabsorbed and re-excreted through theliver into the bile a small fraction is excreted into the urine by the kidney most of them are oxidi-zed to pigments and excreted in the faeces (urobilin, stercobilin) Urobilinogen and bilirubin in urine
Causes of icterus • Icterus (jaundice): bilirubin in the blood exceeds 10 mg/l (hyperbilirubine-mia) bilirubin diffuses into tissues, which become yellow • Pre-hepatic: haemolysis overproduction of bilirubin that exceeds the liver's capacity for handling bilirubin (haemolytic anaemia, neonatal jaundice) unconjugated bilirubin in blood and urobilinogen in urine • Hepatic: liver damage (hepatitis, cirrhosis) capacity for handling bilirubin (uptake, conjugation, excretion) conj. as well as unconj. bilirubin in blood, urobilinogen in urine can if microobstruction is present, otherwise it rises (impaired enterohepatic cycle) • Post-hepatic– obstructive: obstruction of the biliary tree (concretions, tumours) conj. birubin regurgitates into the hepatic veins and lymphatics conj. bilirubin in blood, no urobilinogen in urine
Urobilinogen in urine • Abnormal values: ≥10 mg/l • Causes: • increased degradation of hemoglobin (heavy bleeding, haemolytic jaundice) • liver disease interfering with the enterohepatic urobilinogen cycle (hepatitis, tumours) • Causes of the absence of urobilinogen in the urine: • obstruction in the biliary tree • failure of bile production in the liver • absence of intestinal flora
Direct and indirect bilirubin • Conjugated bilirubin = direct bilirubin x unconjugated = indirect • Normally, only conjugated bilirubin can appear in the urine the level is increased when the plasma concentration of conjugated bilirubin rises • On the other hand, only unconjugated bilirubin can cross BBB (neonatal jaundice encephalopathy can occur)
conj. bilirubin in blood bilirubin is in the urine: liver damage, microobstruction (hepatitis, cirrhosis) Dubin-Johnson Syndrome: defect in the hepatic secretion of conjugated bilirubin into the bile obstructive jaundice unconj. bilirubin in blood bilirubin is NOT in the urine: hemolytic anaemia neonatal jaundice: accelerated haemolysis and immature hepatic system for bilirubin metabolism (low activity of UDP-glucuronosyltransferase) Crigler-Najjar Syndrome: decreased activity of bilirubin UDP-glucuronosyltransferase Bilirubin in blood and urine
Phenylketonuria • Defect in phenylalanine hydroxylase Phe cannot be converted to Tyr, accumulates, and is metabolized to phenylacetate, phenyllactate, and phenylacetylglutamine. Urinary level of phenylpyruvateis elevated. • If leftuntreated, it leads to mental retardation • Prevention: low-Phe diet • Screening: plasma Phe → genetic test
Urolithiasis • Urinary calculi (concretions) are formed in the urinary tract • 80-90% = renal concretions made of calcium salts (oxalate, phosphate) • Factors that predispose to calculi formation: • highly concentrated urine (e.g. dehydration) • increased urinary excretion of: • phosphates, calcium (e.g. increased breakdown of bones) • oxalates • uric acid (hyperuricosuria) • cystine (cystinuria – maybe due to impaired resorption in the kidney) • urine alkalization (in case of excretion of Ca2+, phosphates, oxalates) • urine acidification (pH<5,5) in case of excretion of uric acid
Hyperuricosuria • Excretion of >700-800 mg of uric acid into the urine/24h; serum uric acid rises, too (hyperuricemia) • Causes: • gout • cancer, especially if treated with cytostatic drugs or radiation therapy (increased cell death and thus also increased NA degradation) • renal disease • high intake of purines in the diet • dehydration
Gout • Enzyme defect in PRPP-synthase or HGPRTase overproduction of purines, and thereby also of uric acid crystallization of urates in soft tissues and joints inflammation (arthritis). • Therapy: allopurinol – converted by xanthine oxidase to alloxanthine that inhibits the enzyme synthesis of uric acid, more soluble xanthine and hypoxanthine are excreted
PRPPS and HGPRT in purine metabolism (first step) („salvage pathway“)
Urine sediment • Urine sediment: • substances discharged from organs • crystals (oxalates, urates, phosphates) • Examination detects the presence of: • blood – erythrocyturia (>5 ery/µl); causes: impaired permeability of glomerular membrane, infection, urolithiasis… • leukocytes – pyuria (>10 leuko/µl); causes: infection of the urinary tract • casts – formed in the kidney (the matrix is made of the protein produced by tubules, other components: plasma proteins, lipid droplets) casts can indicate a renal disease (different types of casts indicate different types of damage) • epithelial cells • microorganisms
macrophage hyaline cast erythrocytes a…granulocyte; b…bacteria
hyaline cast cuboidal epithelial cell a…tubular epithelial cell (inside a cast) b…2 cells of a transitional epithelium
granular cast waxy cast (with the cells of tubularepithelium inside)
fatty cast granulocyte yeast yeast