Download
1 / 32
330 likes | 539 Vues
Obstructive disorders of the Urinary system. Medical Management -Diagnostic Tests: KUB, Renal Ultrasound, blood chemistries, endoscopy -Establish urinary drainage Indwelling catheter Suprapubic Cystostomy Ureterostomy Nephrostomy Stent Insertion

E N D
Medical Management • -Diagnostic Tests: KUB, Renal Ultrasound, • blood chemistries, endoscopy • -Establish urinary drainage • Indwelling catheter • Suprapubic Cystostomy • Ureterostomy • Nephrostomy • Stent Insertion • Relieve pain- narcotics, anticholinergics
Nursing Interventions • - observe for signs of hematuria • - aseptic care of the surgical site • -note restoration of urinary function • -provide safe environment to prevent • injury or infection
Etiology/pathophysiology • -Causes: Kinks, cysts, tumors, calculi, • prostatic hypertrophy • -May lead to infection that thrives due to • urine stasis • -May lead to ischemia due to • compression or atrophy of renal tissue • -Clinical Manifestations/Assessment • -Continuous need to void • -Voiding small amounts frequently • -Pain • -Nausea
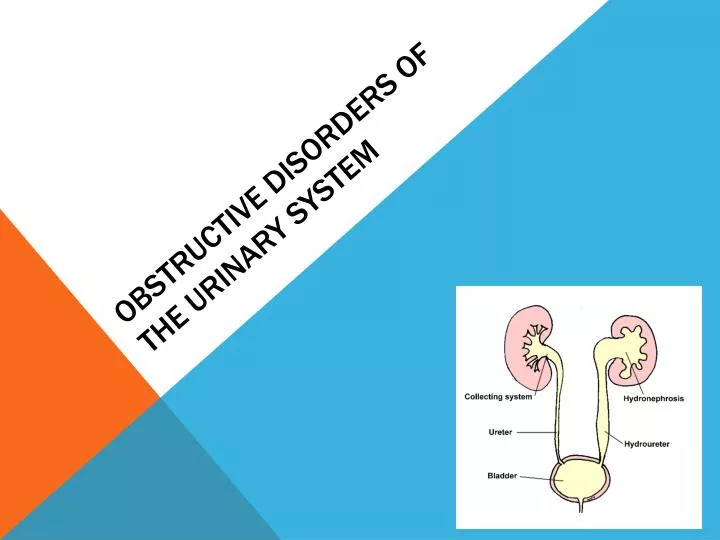
Hydronephrosis • Etiology/Pathophysiology: • -Dilation of the renal pelvis-can be congenital or • develop at any time • -Unilateral or bilateral • -Due to the obstruction of the urinary tract • -The obstruction builds up pressure from the • accumulation of urine that can’t flow past it • -The pressure may cause functional and anatomical • damage to the renal system. • -- The renal pelvis and ureters dilate • --Pressure causes fibrosis and loss of function • of affected nephrons causing kidney • obstruction • _
Clinical Manifestations: • -Dull flank pain (slow onset) • A degree of pain will depend on the • stretching of the urinary tract structures • -Severe stabbing pain (sudden onset) • -Nausea/Vomiting • -Frequency, dribbling, burning and difficulty • starting urination
Medical Management • -Diagnostic Tests: UA, Renal function • studies (BUN, Creatinine), cystoscopy, • IVP, KUB, CT, US • -Surgery to relieve obstruction • -Nephrectomy- if kidney is severely • damaged • -Antibiotics • -Narcotics/antispasmodics
Nursing interventions • -Assessment: Subjective-pain, voiding • pattern, history of obstructive disorders • -Objective-vomiting, hematuria, edema, • urine output, abdominal mass, bladder • distention, tenderness over kidneys/bladder • -Administer meds as ordered, I & O, • observe for signs of infection, vital signs, • pain assessment, encourage intake of • 2L/day unless restricted, anchor drainage • tubes, catheter care • -if surgery is done: incision observation, • care and dressing changes as ordered • -Patient and family teaching
Urolithiasis (kidney stone) Etiology/Pathophysiology -Calculi develop from minerals that have precipitated out of solution and adhere, forming stones that vary in size and shape -Why do these stones form? Not sure! -Contributing factors: predisposed, diet, meds -Identified according to location: nephrolithiasis, ureterolithiasis, cystolithiasis
Clinical Manifestations/Assessments • -Flank or pelvic pain • -Nausea/vomiting • -Hematuria • Medical management • -Diagnostic tests: KUB, IVP, US, Cystoscopy, • UA, etc. • -Medication: antibiotics, analgesics • -Fluids • -Ambulation (if possible) • -Surgical procedures: cystoscopy, • ureterolithotomy, nephrolithotomy
-Lithotripsy- “ extracorporeal shock wave” • -Pt is submerged in a special tank of • water • -Ultrasonic shock waves are used to • pulverize the stone • -Urine still must be strained • -Pt. may still experience renal colic as • the stone fragments pass.
Nursing Interventions • -Assessment • Subjective-pt.’s pain description • Objective-presence of hematuria, nausea, • vomiting, restlessness • - Strain all urine and observe characteristics • -Daily fluid intake of 2L (unless • contraindicated) • -Medication: drug therapy will be specific • to the stone composition • -Administer analgesics • -Monitor lab and diagnostic test results, • especially BUN and Creatinine • -Pt. and family teaching- hydration, dietary • modifications, medication administration, exercise, • keep follow up appointments with MD and when to • contact the MD.
Renal tumors • Etiology/Pathophysiology • -Mostly adenocarcinomas • -Usually develop unilaterally • -Renal cell carcinomas, as a primary • malignant tumor, arise from cells of the • proximal convoluted tubules • Risk factors • -Smoking • -Family history • -Pre-existing renal disorders, such as • polycystic kidney disease and renal cystic • disease secondary to renal failure • -Transitional cell tumors of the renal pelvis • cause hematuria and can be confirmed by • cytological study.
Clinical manifestations • -Early- intermittent painless hematuria • -Late- weight loss, dull flank pain, • palpable mass in flank area, gross • hematuria • Medical management • -Radical Nephrectomy • -Radiation • -Chemotherapy
Nursing Interventions • -Assessment • Subjective-Inquire about blood in the • urine, pain, weight loss, fatigue • Objective-Physical assessment, hematuria • -Adequate hydration to reduce the • discomfort when voiding • -Administer analgesia • -Encourage active/ passive ROM exercises • -Pt./family teaching: community resources, • support groups, home health care, • importance of follow-up care
Renal Cysts • Etiology/Pathophysiology • -A single cyst may not matter, but • multiple cysts interfere with kidney • function • -The most significant problem arise with • polycystic kidney disease (PKD) • -Cysts form in the kidney and can cause • pressure on the kidney structure and • compromise function • -A patient with a long standing renal • insufficiency or a dialysis pt. may • develop PKD
Clinical Manifestations • -Determined by the degree of kidney structure • involved • -Abdominal and flank pain • -Voiding disturbances • - Recurrent UTIs • -Hematuria • -Hypertension
Medical management • -Diagnostic Tests: Radiographic imaging, • blood work • -No specific treatment • -Pain relief • -Heat (unless bleeding) • -Analgesics • -Antibiotics • -Antihypertensives • -Dialysis • -Renal transplant
Nursing Interventions • -Assessment- • Subjective: Abdominal/flank pain, • headaches, GI complaints, voiding • disturbances, history of recurrent UTIs • Objective: Monitor BP, check for hematuria, • note the pt.’s complaints and response to • treatment. • -Patient/family information about genetic • counseling • -Severity of the disease and patient • complaints will determine the nursing • intervention
Tumors of the Urinary Bladder • Etiology/Pathophysiology • -Most common site of cancer in the • urinary tract • -Ranges from benign papilloma to • invasive carcinoma • Clinical Manifestations • -Painless intermittent hematuria • -Changes in voiding pattern
Medial management • -Localized tumor: remove by burning • (fulguration) • -Invasive lesion- partial or total • cystectomy • (Surgery will include diversion such as • an ileal conduit) • Nursing Interventions • -Assess voiding patterns • -Observe characteristics of urine • -Importance of follow-up care
Conditions affecting the prostate gland • BPH- Benign Prostatic Hypertrophy • Etiology/Pathophysiology • -enlargement of the prostate gland which • encircles the urethra at the base of the • bladder • -pressure on the urethra prevents complete • emptying of the bladder • -function of the prostate gland is to secrete • an alkaline fluid that helps to neutralize • seminal fluid and increase sperm motility • -common in men over 50 years old
Clinical manifestations • -Frequent urination • -Difficulty starting urination • -Dysuria • -Frequent UTIs • -Hematuria • -Oliguria • -Nocturia
Medical management • -Diagnostic Test: blood chemistries, • measuring residual urine by cystoscopy, • IVP, rectal exam, cytological evaluation • -Relieve obstruction- foley catheter • -Medication to shrink prostate gland • -Prostatectomy • -Post-Operative: TURP- bladder • irrigations • -urine will be pink to red colored • -Suprapubic/abdominal catheter: assess • drainage
Transurethral • Resection of the • Prostate (TURP)
Nursing Interventions • -Assessment • Subjective- inquire about urine stream, • difficulty starting, frequency, nocturia • Objective-voiding pattern • -Insertion of a foley catheter as ordered, • avoid a rapid decompression (after 1000 ml • is drained, wait 5 minutes before proceeding • to drain more) • -Post-op TURP: maintain patency of foley • catheter and bladder irrigation system, vital • signs, close monitoring of urine for signs of • hemorrhaging • -Medicate for pain and bladder spasms • -Patient/family education