Download
1 / 105
1.08k likes | 1.49k Vues
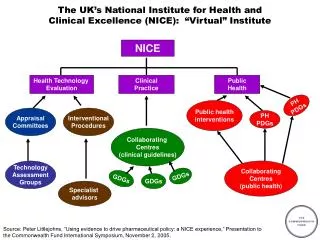
COPD, NICE and the National Clinical Strategy. Harold Hosker Airedale Hospital March 2010. Inflammation.

E N D
COPD, NICE and the National Clinical Strategy Harold Hosker Airedale Hospital March 2010
Inflammation • COPD is a disease state characterised by airflow limitation that is not fully reversible. The airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases • Chronic inflammation is caused by increased numbers of activated inflammatory cells, specifically neutrophils, which can damage lung structure and lead to mucosal oedema and airway narrowing
The impact of COPD • More than 30,000 deaths annually in the UK • UK – 900,000 diagnosed patients • Allowing for underdiagnosis, the true number of patients with COPD in England and Wales is likely to be around 1.5 million • Currently the fifth greatest cause of mortality worldwide – over 2.5 million deaths in 2000 • By 2020, COPD will be the third leading cause of mortality • Exacerbations have an impact on patient quality of life and can be life-threatening
The typical COPD patient • Generally over 40 years • A smoker or ex-smoker • Presentation with: • cough • excessive sputum production • shortness of breath / wheeze
COPD is a heterogeneous disease • Spectrum of clinical disease from ‘pink puffer’ to ‘blue bloater’ • Several different pathological processes
- Protease inhibitors Inflammatory mechanisms in COPD Cigarette smoke ? CD8+ lymphocyte Alveolar macrophage Neutrophil chemotatic factors, cytokines (IL-8) mediators (LTB4) Neutrophil Neutrophil elastase Proteases 1-antitrypsin Alveolar wall destruction (emphysema) mucus hypersecretion (chronic bronchitis)
What is Spirometry? Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Why Perform Spirometry? Measure airflow obstruction to help make a definitive diagnosis of COPD Confirm presence of airway obstruction Assess severity of airflow obstruction in COPD Detect airflow obstruction in smokers who may have few or no symptoms Monitor disease progression in COPD Assess one aspect of response to therapy Assess prognosis (FEV1) in COPD Perform pre-operative assessment
Spirometry – Additional Uses Make a diagnosis and assess severity in a range of other respiratory conditions (eg ILD, MND, G-B) Distinguish between obstruction and restriction as causes of breathlessness Screen workforces in occupational environments Assess fitness to dive Perform pre-employment screening in certain professions
Types of Spirometers • Bellows spirometers: Measure volume; mainly in lung function units • Electronic desk top spirometers: Measure flow and volume with real time display • Small hand-held spirometers: Inexpensive and quick to use but no print out
Lung Volume Terminology Inspiratory reserve volume Inspiratory capacity Total lung capacity Tidal volume Expiratory reserve volume Vital capacity Residual volume
Standard Spirometric Indices • FEV1 - Forced expiratory volume in one second: The volume of air expired in the first second of the blow • FVC - Forced vital capacity: The total volume of air that can be forcibly exhaled in one breath • FEV1/FVC ratio: The fraction of air exhaled in the first second relative to the total volume exhaled • VC - Vital capacity: A volume of a full breath exhaled in the patient’s own time and not forced. Often slightly greater than the FVC, particularly in COPD
Normal Trace Showing FEV1 and FVC FVC 5 4 FEV1 = 4L FVC = 5L FEV1/FVC = 0.8 Volume, liters 3 2 1 1 2 3 4 5 6 1 Time, seconds
Spirogram Patterns Normal Obstructive Restrictive Mixed Obstructive and Restrictive
Predicted Normal Values Affected by: • Age • Height • Sex • Ethnic Origin
Criteria for Normal Post-bronchodilator Spirometry FEV1: % predicted > 80% FVC: % predicted > 80% FEV1/FVC: > 0.7
Spirometry: Obstructive Disease 5 4 Normal 3 Volume, liters FEV1 = 1.8L FVC = 3.2L FEV1/FVC = 0.56 2 Obstructive 1 1 2 3 4 5 6 Time, seconds
Diseases Associated With Airflow Obstruction • COPD • Asthma • Bronchiectasis • Cystic Fibrosis • Sarcoidosis • Lung cancer (greater risk in COPD) • Obliterative Bronchiolitis
Spirometry: Restrictive Disease Normal 5 4 3 Volume, liters Restrictive FEV1 = 1.9L FVC = 2.0L FEV1/FVC = 0.95 2 1 1 2 3 4 5 6 Time, seconds
Diseases Associated with a Restrictive Defect Pulmonary • Fibrosing lung diseases • Pneumoconioses • Pulmonary edema • Parenchymal lung tumors • Lobectomy or pneumonectomy Extrapulmonary • Thoracic cage deformity • Obesity • Pregnancy • Neuromuscular disorders • Fibrothorax
Spirometry • In COPD and asthma, spirometry is preferred to peak flow (PEFR) readings • Serial PEFR readings can confirm / exclude variability (asthma) • Chest X-ray excludes other pathologies but does not usually diagnose COPD
Flow Volume Curve Standard on most desk-top spirometers Adds more information than volume time curve Less understood but not too difficult to interpret Better at demonstrating mildairflow obstruction
Flow Volume Curve Maximum expiratory flow (PEF) Expiratory flow rate L/sec FVC RV TLC Inspiratory flow rate L/sec Volume (L)
Bronchodilator Reversibility Testing • Provides the best achievable FEV1(and FVC) • Helps to differentiate COPD from asthma Must be interpreted with clinical history - neither asthma nor COPD are diagnosed on spirometry alone
Bronchodilator Reversibility Testing in COPD • Results • An increase in FEV1 that is both greater than 200 ml and 12% above the pre-bronchodilator FEV1 (baseline value) is considered significant • It is usually helpful to report the absolute change (in ml) as well as the % change from baseline to set the improvement in a clinical context
Equipment Maintenance Most spirometers need regular calibration to check accuracy Calibration is normally performed with a 3 litre syringe Some electronic spirometers do not require daily/weekly calibration Good equipment cleanliness and anti-infection control are important; check instruction manual Spirometers should be regularly serviced; check manufacturer’s recommendations
Other lung function tests • Lung volumes • Helium dilution, body box (plethysmography) • TLC (RV derived) • Gas transfer • Single breath carbon monoxide transfer • TLCO and KCO (=TLCO/Va) • Mouth pressures • Indirect measure of muscle / diaphragm strength • Pimax, PEmax
Effect of cigarette smoke on airspaces in mice (scanning EM) A: smoke-exposed mice B: matched controls (6 months)
Pathological processes in emphysema • Loss of alveolar surface area • Loss of lung elasticity • Hyperinflation causing mechanical inefficiency • Muscle weakness / cachexia • Small airways collapse • Dynamic hyperinflation
Alveolar wall damage leading to small airways collapse in COPD
Pathological processes in chronic bronchitis • Bronchoconstriction • Airway mucosal inflammation / oedema • Airway remodelling / fibrosis • Mucus hypersecretion • Epithelial / ciliary dysfunction • Ventilation - perfusion mismatch • Hypoxic pulmonary vasoconstriction • Cor pumonale
The role of exacerbations in disease progression • Following an exacerbation, the likelihood of further exacerbation increases • Exacerbations are closely associated with cumulative reduction in health status • High frequency of COPD exacerbations is associated with a rapid decline in lung function and increased risk of hospitalisation • Up to 70% of patients admitted to hospital with an exacerbation are re-admitted within a year
The British Thoracic Society (BTS) guidelines for the management of COPD 1997 Global Strategy for the Diagnosis, Management and Prevention of COPD (GOLD), last update in 2001 and are constantly under peer review (www.goldcopd.com) NICE guidelines were published in 2004, due for revision 2010 COPD Guidelines 1. COPD Guidelines Group of the Standards of Care Committee of the BTS.1997. 2. Pauwels RA et al. 2001.
Diagnose COPD Stop Smoking Effective inhaled therapy Pulmonary Rehabilitation NIV Manage exacerbations Multi-disciplinary working NICE/BTS Recommendations