Download
1 / 1
10 likes | 172 Vues
Introduction.

E N D
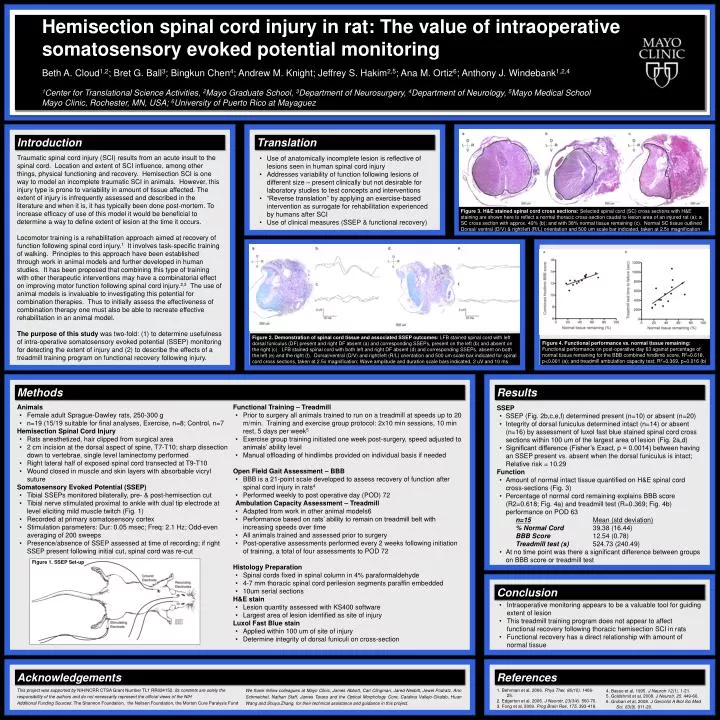
Introduction Traumatic spinal cord injury (SCI) results from an acute insult to the spinal cord. Location and extent of SCI influence, among other things, physical functioning and recovery. Hemisection SCI is one way to model an incomplete traumatic SCI in animals. However, this injury type is prone to variability in amount of tissue affected. The extent of injury is infrequently assessed and described in the literature and when it is, it has typically been done post-mortem. To increase efficacy of use of this model it would be beneficial to determine a way to define extent of lesion at the time it occurs. Locomotor training is a rehabilitation approach aimed at recovery of function following spinal cord injury.1 It involves task-specific training of walking. Principles to this approach have been established through work in animal models and further developed in human studies. It has been proposed that combining this type of training with other therapeutic interventions may have a combinatorial effect on improving motor function following spinal cord injury.2,3 The use of animal models is invaluable to investigating this potential for combination therapies. Thus to initially assess the effectiveness of combination therapy one must also be able to recreate effective rehabilitation in an animal model. The purpose of this study was two-fold: (1) to determine usefulness of intra-operative somatosensory evoked potential (SSEP) monitoring for detecting the extent of injury and (2) to describe the effects of a treadmill training program on functional recovery following injury. Results Methods • SSEP • SSEP (Fig. 2b,c,e,f) determined present (n=10) or absent (n=20) • Integrity of dorsal funiculus determined intact (n=14) or absent (n=16) by assessment of luxol fast blue stained spinal cord cross sections within 100 um of the largest area of lesion (Fig. 2a,d) • Significant difference (Fisher’s Exact, p = 0.0014) between having an SSEP present vs. absent when the dorsal funiculus is intact; Relative risk = 10.29 • Function • Amount of normal intact tissue quantified on H&E spinal cord cross-sections (Fig. 3) • Percentage of normal cord remaining explains BBB score (R2=0.618; Fig. 4a) and treadmill test (R=0.369; Fig. 4b) performance on POD 63 • n=15Mean (std deviation) • % Normal Cord 39.38 (16.44) • BBB Score 12.54 (0.78) • Treadmill test (s) 524.73 (240.49) • At no time point was there a significant difference between groups on BBB score or treadmill test • Animals • Female adult Sprague-Dawley rats, 250-300 g • n=19 (15/19 suitable for final analyses, Exercise, n=8; Control, n=7 • Hemisection Spinal Cord Injury • Rats anesthetized, hair clipped from surgical area • 2 cm incision at the dorsal aspect of spine, T7-T10; sharp dissection down to vertebrae, single level laminectomy performed • Right lateral half of exposed spinal cord transected at T9-T10 • Wound closed in muscle and skin layers with absorbable vicryl suture • Somatosensory Evoked Potential (SSEP) • Tibial SSEPs monitored bilaterally, pre- & post-hemisection cut • Tibial nerve stimulated proximal to ankle with dual tip electrode at level eliciting mild muscle twitch (Fig. 1) • Recorded at primary somatosensory cortex • Stimulation parameters: Dur: 0.05 msec; Freq: 2.1 Hz; Odd-even averaging of 200 sweeps • Presence/absence of SSEP assessed at time of recording; if right SSEP present following initial cut, spinal cord was re-cut • Functional Training – Treadmill • Prior to surgery all animals trained to run on a treadmill at speeds up to 20 m/min. Training and exercise group protocol: 2x10 min sessions, 10 min rest, 5 days per week5 • Exercise group training initiated one week post-surgery, speed adjusted to animals’ ability level • Manual offloading of hindlimbs provided on individual basis if needed • Open Field Gait Assessment – BBB • BBB is a 21-point scale developed to assess recovery of function after spinal cord injury in rats4 • Performed weekly to post operative day (POD) 72 • Ambulation Capacity Assessment – Treadmill • Adapted from work in other animal models6 • Performance based on rats’ ability to remain on treadmill belt with increasing speeds over time • All animals trained and assessed prior to surgery • Post-operative assessments performed every 2 weeks following initiation of training, a total of four assessments to POD 72 • Histology Preparation • Spinal cords fixed in spinal column in 4% paraformaldehyde • 4-7 mm thoracic spinal cord perilesion segments paraffin embedded • 10um serial sections • H&E stain • Lesion quantity assessed with KS400 software • Largest area of lesion identified as site of injury • Luxol Fast Blue stain • Applied within 100 um of site of injury • Determine integrity of dorsal funiculi on cross-section Conclusion • Intraoperative monitoring appears to be a valuable tool for guiding extent of lesion • This treadmill training program does not appear to affect functional recovery following thoracic hemisection SCI in rats • Functional recovery has a direct relationship with amount of normal tissue References Acknowledgements 1. Behrman et al, 2006. Phys Ther, 86(10). 1406-25. 2. Edgerton et al, 2006. J Neurotr, 23(3/4). 560-70. 3. Fong et al, 2009. Prog Brain Res, 175. 393-418. 4. Basso et al, 1995. J Neurotr 12(1). 1-21. 5. Goldshmit et al, 2008. J Neurotr, 25. 449-66. 6. Groban et al, 2008. J Gerontol A Biol Sci Med Sci, 63(9). 911-20. This project was supported by NIH/NCRR CTSA Grant Number TL1 RR024152. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH Additional Funding Sources: The Shannon Foundation, the Neilsen Foundation, the Morton Cure Paralysis Fund We thank fellow colleagues at Mayo Clinic, James Abbott, Carl Clingman,Jared Nesbitt, Jewel Podratz, Ann Schmeichel, Nathan Staff, James Tarara and the Optical Morphology Core,Catalina Vallejo-Giraldo, Huan Wang and Shuya Zhang, for their technical assistance and guidance in this project. Hemisection spinal cord injury in rat: The value of intraoperative somatosensory evoked potential monitoring Beth A. Cloud1,2; Bret G. Ball3; Bingkun Chen4; Andrew M. Knight; Jeffrey S. Hakim2,5; Ana M. Ortiz6; Anthony J. Windebank1,2,4 1Center for Translational Science Activities, 2Mayo Graduate School, 3Department of Neurosurgery, 4Department of Neurology, 5Mayo Medical School Mayo Clinic, Rochester, MN, USA; 6University of Puerto Rico at Mayaguez Translation • Use of anatomically incomplete lesion is reflective of lesions seen in human spinal cord injury • Addresses variability of function following lesions of different size – present clinically but not desirable for laboratory studies to test concepts and interventions • “Reverse translation” by applying an exercise-based intervention as surrogate for rehabilitation experienced by humans after SCI • Use of clinical measures (SSEP & functional recovery) Figure 3. H&E stained spinal cord cross sections: Selected spinal cord (SC) cross sections with H&E staining are shown here to reflect a normal thoracic cross-section caudal to lesion area of an injured rat (a); a SC cross section with approx. 49% (b); and with 38% normal tissue remaining (c). Normal SC tissue outlined Dorsal/ ventral (D/V) & right/left (R/L) orientation and 500 um scale bar indicated, taken at 2.5x magnification Figure 2. Demonstration of spinal cord tissue and associated SSEP outcomes: LFB stained spinal cord with left dorsal funiculus (DF) present and right DF absent (a) and corresponding SSEPs, present on the left (b) and absent on the right (c). LFB stained spinal cord with both left and right DF absent (d) and corresponding SSEPs, absent on both the left (e) and the right (f). Dorsal/ventral (D/V) and right/left (R/L) orientation and 500 um scale bar indicated for spinal cord cross sections, taken at 2.5x magnification; Wave amplitude and duration scale bars indicated, 2 uV and 10 ms Figure 4. Functional performance vs. normal tissue remaining: Functional performance on post-operative day 63 against percentage of normal tissue remaining for the BBB combined hindlimb score, R2=0.618, p<0.001 (a); and treadmill ambulation capacity test, R2=0.369, p=0.016 (b) Figure 1. SSEP Set-up