Download
1 / 22
320 likes | 4.32k Vues
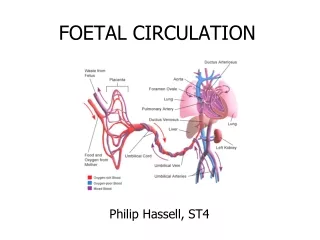
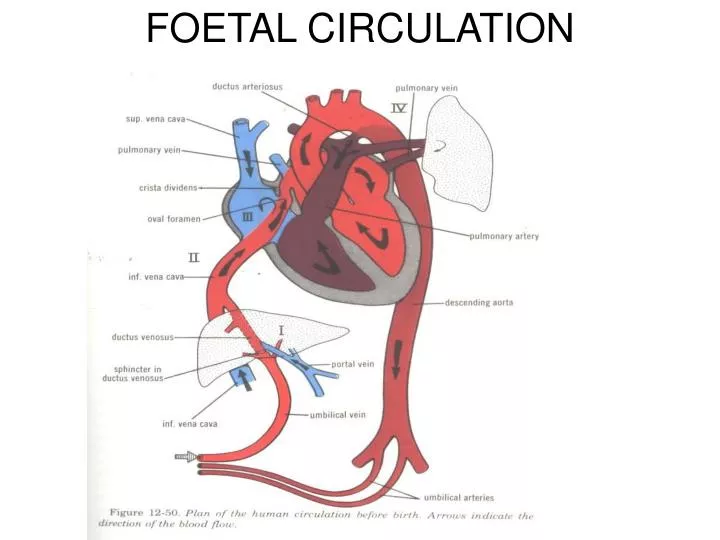
FOETAL CIRCULATION. CIRCULATION AFTER BIRTH. EMBRYOLOGY.

E N D
EMBRYOLOGY • Embryologically, the septum primum separates the two atria first, moving inferiorly toward the endocardial cushions. The ventricular septum forms by moving upward from the ventricles to the endocardial cushions at the same time. If the atrial septum does not make it all the way, the residual defect in the septum primum (ostium primum) results in the primum ASD. • If the septum primum makes it all the way, a hole or holes (fenestrations) form in the middle of the septum (forming the ostium secundum). A second septum then moves down the right side of the first and normally covers the ostium secundum hole. If it does not cover the hole, a secundum ASD is present. • The septum secundum normally completely covers the right side of the atrial septum except for an ovale hole in it (the foramen ovale). If the septae do not fuse, a patent path from the RA to the LA persists (the patent foramen ovale PFO). • The most common form of ASD (80% of cases) is persistence of the ostium secundum in the mid septum; less commonly, the ostium primum (which is low in the septum) persists • .
ATRIAL WAVES • a= atrial contraction • c= contraction of ventricle and closure of tricuspid valve • x=x descent • v=venous filling • y= y descent due to opening of tricuspid valve
Essentials of Diagnosis • Often asymptomatic and discovered on routine physical examination. • RV lift; S2 widely split and fixed. • Grade IIII/VI systolic ejection murmur at pulmonary area. • ECG shows RV conduction delay; • radiograph shows dilated pulmonary arteries and increased vascularity; echocardiography/Doppler diagnostic. • A PFO is present in 25% of the population but can lead to paradoxical emboli and cerebrovascular events. Suspicion should be highest in patients who had cryptogenic stroke before age 55. • In all cases, normally oxygenated blood from the higher-pressure LA passes into the RA, increasing RV output and pulmonary blood flow. In children, the degree of shunting across these defects may be quite large (3:1 or so). As the RV diastolic pressure rises from the chronic volume overload, the RA pressure may rise and the degree of left-to-right shunting may decrease. Eventually, the shunt may even be right-to-left and cyanosis appears
CHAMBER PRESSURES • Simultaneous left and right atrial and differential pressure across an atrial septal defect. The pressure difference across the defect is greatest before the v wave. The right atrial pressure tracing is inverted because it is recorded by a differential manometer
SYMPTOMS AND SIGNS • Patients with small or moderate ASDs and with a PFO are asymptomatic unless a complication occurs. • With large shunts, exertional dyspnoea or cardiac failure may develop, most commonly in the fourth decade of life or later. • Prominent RV and PA pulsations are readily visible and palpable. • A moderately loud systolic ejection murmur can be heard in the second and third interspaces parasternally as a result of increased PA flow. • S2 is widely split and does not vary with breathing due to the fact that the left-to-right shunt decreases as the RA pressure increases with inspiration
EISENMENGER COMPLEX • The pulmonary pressures are modestly elevated in most patients with an ASD due to the high pulmonary blood flow, but severe pulmonary hypertension (Eisenmenger's complex) is actually rare, occurring in only about 15% of the patients (see illustration). • Eventual RV failure may occur, and most shunts should be corrected unless they are quite small (< 1.5:1 right-to-left shunt). In adults, a large right-to-left shunt may have begun to reverse, so the absolute size at the time the patient is studied may underestimate what it was some years ago. In addition, • in most patients the LV compliance normally declines more over time than the RV, and the natural history of small atrial septal shunts is to increase as the patient ages (unless RV failure ensues).
ECG IN ASD • Right axis deviation or RVH may be present depending on the size of the RV volume overload (see ECG); (see ECG). Incomplete or complete right bundle branch block is present in nearly all cases of ASD, and superior axis deviation is noted in the AV canal defect, where complete heart block is often seen as well. With sinus venosus defects, the P axis is leftward of +15 due to abnormal atrial activation with loss of the upper RA tissue from around the sinus node
XRAY IN ASD • The chest radiograph shows large pulmonary arteries, increased pulmonary vascularity, an enlarged RA and RV, and a small aortic knob with all pre-tricuspid cardiac left-to-right shunts.
DIAGNOSTIC STUDIES • Echocardiography demonstrates evidence of RA and RV volume overload. The atrial defect is usually observed, though sinus venosus defects may be elusive. • Many patients with a PFO also have a redundant atrial septum (atrial septal aneurysm) that promotes right-to-left shunting. Echocardiography with agitated saline bubble contrast can demonstrate a right-to-left shunt and both pulsed and colour flow Doppler flow studies can demonstrate shunting in either direction (see Video). A TEE is helpful when transthoracic echocardiography quality is not optimal, and it improves the sensitivity for small shunts and provides a better assessment of PFO anatomy. Radionuclide flow studies quantify left-to-right shunting by observing the bolus of contrast within the lung fields and demonstrating early recirculation. Both CT and MRI can also elucidate the atrial septal anatomy as well, and allow for observation of associated lesions. Cardiac catheterization is often helpful, especially if there are associated anomalous pulmonary veins. The size and location of the shunt can be determined and the pulmonary pressure and pulmonary vascular resistance (PVR) measured (see ECG). Cardiac catheterization is required if percutaneous closure is to be contemplated
Prognosis & Treatment • Patients with small atrial shunts may live a normal life span. Large shunts usually cause disability by age 40 years. Because left-to-right shunts tend to increase with age-related changes in LV compliance, most clinicians believe that closure of all shunts over 1.5:1 should be accomplished. • Increased PVR and hypertension secondary to pulmonary vascular disease rarely occur in childhood or young adult life in secundum defects but are more common in primum defects. Significant pulmonary hypertension rarely develops in older patients. After age 40 years, cardiac arrhythmias (especially atrial fibrillation) and heart failure may occur due to the chronic right heart volume overload. • Paradoxical systemic arterial embolization becomes more of a concern as RV compliance is lost and the left-to-right shunt begins to reverse. • PFOs are not associated with significant shunting, and therefore the patients are asymptomatic and the heart size is normal. However, PFOs are responsible for most paradoxical emboli and are one of the most frequent causes of cryptogenic strokes in patients under age 55 years. That is likely because there is often right-to-left or bidirectional shunting, and the IVC blood is directed toward the foramen ovale by the eustachian valve.
Intervention • Small ASDs do not require intervention. The easiest way to decide if a shunt is small is by echocardiography. If the shunt is not creating an RV volume overload, then one can assume the shunt needs no further evaluation. • For larger deficits (those with an RV volume overload), surgery can be done at very low risk. • Surgery involves anything from simple stitching of the foramen closed to patching of the hole with Dacron or a pericardial patch. Anomalous pulmonary venous connections are baffled to the LA through the sinus venosus defect when such anomalous veins are present. • For ostium secundum ASDs, percutaneous closure by use of a variety of devices is now preferred over surgery. The percutaneous closure devices often resemble double umbrellas that lock the septum between the Dacron umbrellas when opened
PFO • Patients with a PFO may have symptoms related to stroke or transient ischemic attack (especially if the age is under 55) or have hypoxemia (especially upon standing so called platypnea orthodeoxia). • There are data that suggest that migraine headaches may be more common in patients with a PFO, suggesting some unknown substance normally metabolized in the lung is entering the systemic circulation through the PFO. • For patients with cryptogenic stroke or transient ischemic attack, it is uncertain whether closure of the PFO, either by open surgical or percutaneous techniques, has any advantage over anticoagulation with either warfarin or aspirin. Although there are no data yet suggesting that PFO closure is better than medical therapy, ongoing randomized trials should help settle this issue.