Download
1 / 12
120 likes | 332 Vues
D.I.Ivanovsky 1864- 1920. ANALYSIS OF CASES OF HEPATITIS E INFECTION WITH SUSPECTED HCV CO-INFECTION. NATALIA V. PETRAKOVA D.I.IVANOVSKY INSTITUTE OF VIROLOGY. Basics. D.I.Ivanovsky 1864- 1920.

E N D
D.I.Ivanovsky 1864- 1920 ANALYSIS OF CASES OF HEPATITIS E INFECTION WITH SUSPECTED HCV CO-INFECTION NATALIA V. PETRAKOVA D.I.IVANOVSKY INSTITUTE OF VIROLOGY
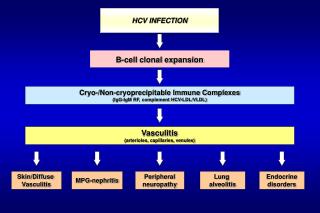
Basics D.I.Ivanovsky 1864- 1920 • Hepatitis E Virus (HEV) causes acute epidemic & sporadic infectious hepatitis - BUT endemic for Asia, Middle East & Africa- An increase displayed recently of non-travel- associated HEV infections in Europe & Japan- HEV is often detected in pts with acute liver disease - Frequently as co-infection with HBV & HCV - Correlations were found of HEV infection (HEV RNA and/or anti-HEV antibodies) and HBV & HCV viremia
Report D.I.Ivanovsky 1864- 1920 Here we present 3 cases of acute HEV infection associated with immune imprints of hepatitis C virus strongly indicating a concomitant resolving HCV infection in pts from the region non-endemic for HEV who had no known risk factors for HEV transmission
PATIENTS D.I.Ivanovsky 1864- 1920 Three pts (Z., M., T.) were admitted to the Department of Hepatology, Infectious Diseases Hospital nr1, Moscow, Russia with clinical picture of acute hepatitis (in details – in the report of E. Tsiganova)NB! The results of routine laboratory investigations for HAV, HBV and HCV were negative. Analysis for HEV is not done routinely! After basic symptomatic treatment, patients were discharged with the diagnosis of acute hepatitis of unknown etiology, and advised to come for a follow-up in six months. Follow-up performed on week 30 showed normal physiological parameters, blood cell counts and biochemistry
RETROSPECTIVE INVESTIGATION D.I.Ivanovsky 1864- 1920 Due to diagnosis of acute hepatitis of unknown etiology sera collected at weeks 1, 2 and 30 (from pts Z. & T.) and sample from week 1 (pt M.) were subjected to extended retrospective investigation. All sera were positive for HEV IgG; sera collected at weeks 1, 2 were also positive for anti-HEV IgM (Vector Best, Novosibirsk, Russia). Serum Z. from week 2 contained HEV RNA (in house PCR by Dr. M. Michailov). Additional serological and molecular testing for HAV, HBV, HCV, HGV, HHV-1, 2, 6 and 8, EBV, CMV, TTV, parvovirus B19 gave negative results. However, the re-evaluation HCV ELISA and Immunoblot analysis for samples collected at week 1 and 2 (but not week 30) showed signal to be within “10% grey zone”/ indeterminate.
DETAILED INVESTIGATION FOR HCV D.I.Ivanovsky 1864- 1920 To decipher the indeterminate anti-HCV seroreactivity, sera were screened for the presence of antibodies to a panel of HCV antigens including recombinant - HCV core - E1, E2 - NS5B- NS3, NS4, NS5A (Diagnostics Systems, Niznii Novgorod, Russia)and synthetic peptides derived from regions- core - NS3 of HCV 1b- HVR-N and HVR-C (two consensus peptides ftom the N- and C-terminal regions of hypervariable loop 1 of E2 Serology was done by indirect ELISA on Maxisorb plates (Nunc) using HRP-labeled goat anti-human antibodies. Optical density (OD) cut-off values for each HCV antigen were set as the average OD demonstrated by serum samples of healthy individuals (n=7) plus 3 SDs.
GROUPS FOR COMPARISON D.I.Ivanovsky 1864- 1920 - HUNO/HEV positive – 7 sera from 3 pts as a MAIN GROUP Groups for comparizon :- HEV – 5 individual sera- HCV – 8 sera (1 acute pt in dynamics)- HUNO/HEV negative – 3 individual sera
DISCOVERED SEROREACTIVITY D.I.Ivanovsky 1864- 1920 - Sera from the acute period contained antibodies against both - structural - core, E2 - non-structural (NS3, NS5a) HCV proteins in titers from 200 to >2400 - Most of the antibody response was, however, short-living - All patients sera were negative for antibodies against control proteins and peptides
OVERALL ANTIBODY REACTIVITY Signal is ratio OD/cut-off (average of 7 normal sera + 3 SDs) Cross-point is 1.1 and negative & “grey zone” are below axis D.I.Ivanovsky 1864- 1920 HUNO/HEV positive HCV positive 1 2 3 1 2 3 Healthy HEV 1 2 3 1 2 3
SEROREVERSION & NARROWING OF EPITOPE SPECIFICITY D.I.Ivanovsky 1864- 1920
CONCLUSIONS D.I.Ivanovsky 1864- 1920 - In three pts with acute HEV infection (total 7 sera) the seroreactivity was revealed against several structural & non-structural Ags- The profile of this reactivity is very characteristic for acute self-limiting HCV infection : - - seroreversion/signal drop down/loss of Abs with time - - narrowing of epitope specificity/loss of recognition of individual peptides- Revealed seroreactivity is not cross-reactive or unspecific due to the acute period of HEV infection as in control HEV group acute serum didn’t give these reactions
Institute of Microbiology, Tumor and Cell Biology, Karolinska Institutet, Stockholm, Sweden Maria Isaguliants D.I. Ivanovsky Institute of Virology, Moscow, Russia Natalia Petrakova Elena Tsyganova Moscow State University of Dentistry and Medicine, Moscow, Russia Olga Znoyko Elena Tsyganova NikolaiYuschuk Swedish Institute for Infectious Disease Control, Stockholm, Sweden Tatjana Tallo National Institute for Health Development, Tallinn, Estonia Tatjana Tallo Valentina Tefanova Chumakov Institute of Polyomyelitis and Viral Encephalitis, Moscow region, Russia Sergey Solonin Karen Kyregyan Olga Isaeva Michail Michailov INSERM, Lyon, France Birke Bartosch DNA Technology, and Institute of Immunology, Moscow, Russia Tatjana Petrova W.A. Engelhardt Institute of Molecular Biology, Moscow, Russia Sergey Kochetkov Malmö University Hospital, Lund University, Malmö, Sweden Anders Widell TEAMS D.I.Ivanovsky 1864- 1920