Download
1 / 32
320 likes | 642 Vues
WORKING WITH BLOOD GASES. Martha Richter MSN, CRNA. OBJECTIVES. This lecture should help you Analyze blood gas results Discuss implications on anesthesia management when states of alkalosis/acidosis exist List the variations in acidosis/alkalosis states. ACID BASE & ABGS.

E N D
WORKING WITH BLOOD GASES Martha Richter MSN, CRNA
OBJECTIVES • This lecture should help you • Analyze blood gas results • Discuss implications on anesthesia management when states of alkalosis/acidosis exist • List the variations in acidosis/alkalosis states
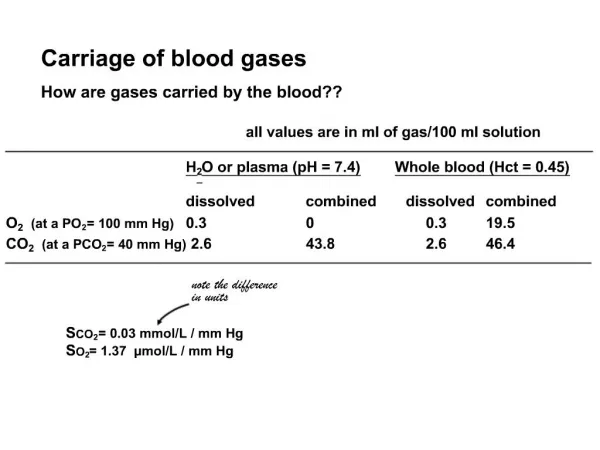
ACID BASE & ABGS • Henderson-Hasselbach’s equation describes the equilibrium between acids & bases • Disturbances • Metabolic – HCO3 • Respiratory- PaCO2 • Ph=(-)log of H ion concentration; describes acidity or alkalinity
ACID BASE & ABG • What are the normal values: • pH- 7.35-7.45 • PaO2 – 90-100 • PaCO2 35-45 • Bic 21-27 mEq/l
ABGS • What are the different states? • Metabolis alkalosis • Metabolis acidosis • Respiratory alkalosis • Respiratory acidosis • Compensated states of the above
METABOLIC ALKALOSIS • pH >7.45 Bic >27 mEq/l • Assoc with increased mortality in the critically ill • Caused by: N/G suction, diuretics, renal hypoperfusion, hypokalemia, hypochloremia
METABOLIC ALKALOSIS • Physiological effects • Hypokalemia + alkalosis = ventricular arrhythmias; potentiates dig. • May generate compensatory hypoventilation, generating hypercarbia = PaO2 dec • Inc bronchial tone + dec vent effort = atelectesis contributor • Oxyhemoglobin dissoc curve shifts to L = dec availability of O2 to tissues • Dec CO
METABOLIC ALKALOSIS • Remember: • the majority of CO2 is carried as bicarb. • The greatest amount of CO2 is eliminated thru the lungs. • Do not compound metabolic alkalosis with respiratory alkalosis! • CV depression • arrhythmias
METABOLIC ALKALOSIS • What are the treatment options? • Volume expansion to inc renal perfusion • K to correct • Consider 0.9NS instead of LR • Administer H • Ammonium cl, arginine HCl, 0.1 N-hydrocholic acid • Acetazolamide (carbonic anhydrase inhibitor-influences renal bicarb wasting) • Acid dialysis
METABOLIC ACIDOSIS • pH <7.35 Bicarb <21 mEq/l • Anion gap calculation • Na-[Cl]+[HCO3]=<13 mEq/l normal • External losses as cause = normal anion gap • Anion gap >13 when:lactic/ketoacidosis, uremic retention of waste products, toxin ingest (ASA, ethylene glycol, methanol)
METABOLIC ACIDOSIS • EFFECTS OF LOW PH • Dec myocardial contractility • Inc pulmonary vasc resist • Increase SVR • Impaired response to catechols by CV system • Normally, the body compensates with hyperventilation. Patients who are unable to compensate in this way may require mechanical ventilation
METABOLIC ACIDOSIS • ASSESS THE PATIENT • RX aimed at correcting the underlying influences • Hypovolemia • Hypoperfusion • How is the renal function • Does any pulmonary pathology interfere with gas exchange
METABOLIC ACIDOSIS • INTRAOP CARE • Art line to facilitate ABG “tracking” • PA catheter • Remember the exaggerated response to drugs & PPV
WHAT ABOUT BICARB RX? • Severe acidosis may require IV NaBicarb • One calc: Wt kgX0.3X(24mEq/l-actual HCO3)/2 This is a half-correction used for the initial dose. Req. ABG recheck at freq intervals. The use of Bicarb remains controversial.
RESPIRATORY ALKALOSIS • pH >7.45 PaCO2 <35 • Response to inc minute volume • Pain • Anxiety • Hypoxemia • CNS disease • Sepsis
RESPIRATORY ALKALOSIS • May produce • Hypokalemia • Hypocalcemia • Dysrhthmias • Bronchoconstriction • Hypotension • Potentiation Dig toxicity
RESPIRATORY ALKALOSIS • Remember the effect on CBF • Acute profound hypocapnia = <20mmHg • Cerebral ischemia! • Rx the underlying cause!
RESPIRATORY ACIDOSIS • pH <7.35 PaCO2 >45 (always) • Causes • Minute vol insuff to eliminate CO2 • CNS depression (drugs/injury) • Increased work of breathing=tired • Airway obstruction • Neuromuscular dysfunction • Inc Vd dut to pulmonary embolism,COPD,acute respiratory failure • Acute/chronic • Increase in CO2 prod
RESPIRATORY ACIDOSIS • When d/t intrinsic pulmonary dis • Remember to “handle with care” • Postop pain management issues • Art line to allow ABG sampling • Aim for a normal pH in CO2 retainers • Acute resp acid requires mechanical vent if the underlying cause can’t be treated quickly
INTERPRETING THE ABG • Need to know the hx, ABG, lytes • Identify what needs immed intervention • Resp acid pH<7.1=vent, ETT • Metabol acid pH<7.1=alkalinizing RX What’s the disturbance? Acidosis/alkalosis resp/metabol/mixed Is it simple resp acute? Low pCO2 should have elev pH with low HCO3.
INTERPRETING THE ABG • A calculation for determining acute condition • pH decreases 0.1 for every 10mm inc PaCO2 • HCO3 dec 2mEq/l for every 10mmHg dec PaCO2 • If your numbers don’t follow this rule, consider a chronic condition • When you can’t describe acute/chronic resp changes, consider metabolic process
COMPENSATION RULES • Respiratory comp occurs more quickly then metabolic • Overcompensation is rare • Inadequate/excess compen suggests additional primary process • Metabolic acidosis assoc with inc anion gap is never compensatory • Rules of thumb approximate pH-H relationship • The presence of an anion gap sorts out the presence of metabolic acidosis
COMPENSATION • Respiratory compensation for metabolic processes happens immediately • Metabolic compensation for respiratory processes happens slowly (1-2 days)
WHY IS THE TEMPERATURE IMPORTANT? • CO2 is more soluble in cold blood. • Request ABGs at true body temp • The difference is important when comparing ABGs with ETCO2 or gas results from pump-oxygenator
REMEMBER THE BASE EXCESS • Base excess • (-) = metabolic component in the face of acidosis • (+)= compensated in the face of acidosis • As BE goes down, reflects cellular hypoperfusion/hypoxia-correct the underlying problem
EXAMPLES • Pure (Uncompensated) Respiratory • Acute • Acidosis: PCO2=52, pH=7.3 • Hypoventilation • Requires 1-2 days for compensation • Alkalosis:PCO2=28, pH=7.5 • Acute hyperventilation • Requires 1-2 days for compensation
EXAMPLES • Compensated Respiratory • Chronic acidosis: pH7.3, PaCO2=64 • COPD • Chronic alkalosis: pH 7.45, PaCO2 – 28 • High altitude response to hypoxia
EXAMPLES • COMPENSATED METABOLIC Acidosis pH 7.3, PaCO2 28 compensation after lactic acidosis Alkalosis pH 7.5, PaCO2 52 comp after vomiting/aspiration
EXAMPLES • MIXED • Acidosis • pH 7.1 PaCO2 64 • Following trauma with tissue ischem &resp depression • Alkalosis • pH 7.6 PaCO2 28 • Gastric aspiration with mechan hyperventilation
RULES OF THUMB Barash • Dec PaCO2 • pH inc 0.1 for every 10 mmHg dec PaCO2 • Bicarb dec 2 mEq/l for every 10 mmHg dec in PaCO2 • pH will nearly normalize hypocarbia is sustainable • Bicarb will dec 5-6 mEq/l for each chronic 10 mmHg dec PaCO2
RULES OF THUMB Barash • Increased PaCO2 • pH will dec 0.05 for every acute PaCO2 inc 10 mmHg • Bicarb will inc 1.0 mEq/l for every PaCO2 inc of 10 mmHg • pH will return toward normal if hypercarbia is sustained • Bicarb will increase 4 mEq/l for ea chronic 10 mmHg inc PaCO2
ACID BASE & ABGS • Be logical in your analysis • Keep it simple