Download
1 / 90
900 likes | 1.22k Vues
Trauma. Zhanfei Li. MD &PhD Associate professor and attending surgeon Division of Traumatic Surgery, TJH. Introduction. Trauma is a major worldwide public health problem. It is one of the leading causes of death and disability in both industrialized and developing countries.

E N D
Trauma Zhanfei Li. MD &PhD Associate professor and attending surgeon Division of Traumatic Surgery, TJH
Introduction • Trauma is a major worldwide public health problem. • It is one of the leading causes of death and disability in both industrialized and developing countries. • In the US, trauma is the 1st cause of death in children and adults <45 years of age. • It is called “the disease of the civilized society”.
Incidence of Trauma Leading cause of death in U.S. in patients less than 45 years old (CDC 2004) 60 million injured 160,000 die – (56/100,000) and the rate is going up 9 million disabled - 300,000 permanently Trauma is more commonly a disease of the young (15-34) thus has a far greater economic impact Significant yearly economic cost
Why do Trauma Patients Die? Some are killed immediately from massive injuries (can’t help these except by prevention) Many die from head injuries---Rapid care can save many of these Many bleed to death bleeding may not be initially recognized These patients may die while waiting for transfer to a trauma hospital Some die later of complications (organ failure or sepsis) Survival is often related to how soon the bleeding was stopped and blood volume restored
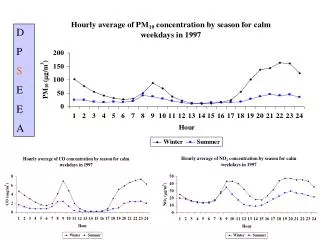
Mortality after traumatic injury • One half of trauma deaths occur within seconds or minutes due to injury of aorta, heart, brain, etc. • Very few of these victims can be saved by trauma systems. • The second mortality peak occurs within hours of injury and accounts for ~30% of deaths. The major causes of deaths are massive hemorrhage and brain injury. • The third mortality peak occurs in 24hours after injury, mainly after 1 week. The major causes are infection, sepsis and MOF.
Tri-modal distribution of injury-related death Within seconds and minutes Three peak of injury-related death Within hours Hemorrhage and brain injury >24hours and later Infection and MOF Golden hour
The Golden Hour 转运 损伤 初始评估 (初步检查) 病情稳定 第一小时 挽救生命的干预 (复苏) 从头到脚评估 (再次检查)
Development of trauma care • Modern trauma care has evolved from the close relation of surgery and casualty management in war. • Many important concepts, including prehospital transport, volume resuscitation, life support and critical care have been advanced based on the observations during war. • The first organized trauma unit opened in 1961 at the University of Maryland. • Trauma care requires collaboration of pre-hospital care, ER, multiple disciplines (general surgery, neurosurgery, orthopaedic surgery, thoracic surgery, vascular surgery, as well as rehabilitation.
A System Saving Lives SURVIVOR OR STATISTIC?
Trauma System • Organized system within a given region including prehospital care, acute hospital care, and rehabilitation
Trauma System A trauma system involves trauma centers working together with 9-1-1, EMTs, ambulances, helicopters, and other health care resources in a coordinated and preplanned way. This network of care is designed to get seriously injured people to the place with the right resources as quickly as possible
Development of trauma care system Components of trauma care rehabilitation First aid Trauma system ER Traumatic surgery/ICU OR Re-evaluation and advanced life support
Why is it important? • Multiple studies show that care in a trauma system has: • Decreased mortality of 10-30% • Reduced disability • Improved quality of care • Cost savings
Trauma Center Trauma centers are selected hospitals that provide a full range of care for severely injured patients 24 hours a day, seven days a week. The trauma care includes ready-to-go teams that perform immediate surgery and other necessary procedures for people with life-threatening injuries, for example, due to car accident, burn, bad fall, or gunshot.
Trauma Center • Hospital that meets certain readiness requirements for care of injured persons • Categorized by level (usually 1 through 4) by capacity/ capability • Involves having the right personnel and equipment readily available for trauma care
How does the System Save Lives? It correctly identifies the patients who need trauma care Anticipates the resources needed to treat the patients Locates the available needed resources Routes the patient “right” the first time to reduce time to appropriate care Arranges interfacility transfers if needed to reduce time to appropriate care Improves care by the QI process and Research activity
Who is a “Trauma System” Patient? A “trauma” patient is any patient who is injured Most injuries are minor and should be treated at a local community hospital Less than 10% of patients with injuries need to go to a trauma center. These are Trauma System patients. A “Trauma System” patient has life-threatening injuries that require rapid, specialized care. Examples are: Injured patients with signs of shock Injured patients with airway problems Head or spinal injuries Multiple long bone fractures Ejection from vehicle Major burns or smaller burns with other injuries
This is an Trauma Patient but not a Trauma System Patient Fracture-Dislocation of the Ankle 骨折-踝关节脱位
What are the Qualities of a GoodTrauma System? Network of hospitals with the commitment and the resources to care for trauma system patients Organized plan to route critical patients to the right hospital that is ready to care for them Constant monitoring of the system to correct problems, improve the system, and validate the quality of care provided
Elements of an Effective Trauma SYSTEM Effective pre-hospital providers and protocols Designated trauma centers (hospitals designated Level 1-4) Trained and available physician trauma specialists and nurses Rehabilitation facilities Trauma registry Continuous quality improvement Communication and coordination Injury Prevention and Control programs
INITIAL EVALUATION AND RESUSCITATIONOF THE INJURED PATIENT Primary Survey • Airway Management with Cervical Spine Protection • Breathing and Ventilation • Circulation with Hemorrhage Control • Disability and Exposure • Shock Classification and Initial Fluid Resuscitation Secondary Survey
Primary survey • Airway Management with Cervical Spine Protection • Breathing and Ventilation • Circulation with Hemorrhage Control • Disability and Exposure • Shock Classification and Initial Fluid Resuscitation • Persistent Hypotension
Initial management of trauma patients CRASH PLAN VIPC ABCDE Principle:the No1 priority is to save the life of patients, the second one is to reserve function of organs
VIPC V: Ventilation I: Infusion P: Pulsation C: Control bleeding
ABCDE VIPC V: Ventilation A=airway B=breath C=circulation D=disability E=exposure for complete examination I: Infusion P: Pulsation C: Control bleeding
Crash Plan Crash Plan C=cardiac P=pelvis R=respiratory L=limb A=abdomen A=arteries S=spine N=nerves H=head
Airway Management with Cervical Spine Protection • Ensuring a patent airway is the first priority in the primary survey. This is essential, because efforts to restore cardiovascular integrity will be futile unless the oxygen content of the blood is adequate. • Simultaneously, all patients with blunt trauma require cervical spine immobilization until injury is excluded. This is typically accomplished by applying a hard collar or placing sandbags on both sides of the head with the patient’s forehead taped across the bags to the backboard.
Airway Management with Cervical Spine Protection • Patients who have an abnormal voice, abnormal breathing sounds, tachypnea, or altered mental status require further airway evaluation. • Cricothyroidotomy is performed through a generous vertical incision, with sharp division of the subcutaneous tissues and strap muscles. Visualization may be improved by having an assistant retract laterally on the neck incision using army-navy retractors.
Cricothyroidotomy • Cricothyroidotomy is recommended for emergent surgical establishment of a patent airway. A. Use of a tracheostomy hook stabilizes the thyroid cartilage and facilitates tube insertion. B. A 6.0 tracheostomy tube or endotracheal tube is inserted after digital confirmation of airway access.
Tracheostomy • Emergent tracheostomy is indicated in patients with laryngotracheal separation or laryngeal fractures, in whom cricothyroidotomy may cause further damage or result in complete loss of the airway
Breathing and ventilation • Once a secure airway is obtained, adequate oxygenation and ventilation must be assured. All injured patients should receive supplemental oxygen and be monitored by pulse oximetry.
Breathing and ventilation • The following conditions constitute an immediate threat to life due to inadequate ventilation and should be recognized during the primary survey: tension pneumothorax open pneumothorax flail chest with underlying pulmonary contusion • All of these diagnoses should be made during the initial physical examination.
Tension pneumothorax • The diagnosis of tension pneumothorax is implied by respiratory distress and hypotension in combination with any of the following physical signs in patients with chest trauma: tracheal deviation away from the affected side lack of or decreased breath sounds on the affected side subcutaneous emphysema on the affected side
Tension pneumothorax • In cases of tension pneumothorax, the paren-chymal tear in the lung acts as a one-way valve, with each inhalation allowing additional air to accumulate in the pleural space. • The normally negative intrapleural pressure becomes positive, which depresses the ipsilateral hemidiaphragm and shifts the mediastinal structures into the contralateral chest.
Tension pneumothorax • Subsequently, the contralat-eral lung is compressed and the heart rotates about the superior and inferior vena cava; • This decreases venous return and ultimately cardiac output, which results in cardiovascular collapse.
Tension pneumothorax • Vital signs differentiate a tension pneumothorax from a simple pneumothorax; each can have similar signs, symptoms, and examination findings, but hypotension qualifies the pneumothorax as a tension pneumothorax.
Tension pneumothorax-therapy • Although immediate needle thoracostomy decompression with a 14-gauge angiocatheter in the second intercostal space in the midclavicular line may be indicated in the field, tube thoracostomy should be performed immediately in the ED before a chest radiograph is obtained
Open pneumothorax • An open pneumothorax or “sucking chest wound” occurs with full-thickness loss of the chest wall, permitting free communication between the pleural space and the atmosphere. • This compromises ventilation due to equilibration of atmospheric and pleural pressures, which prevents lung inflation and alveolar ventilation, and results in hypoxia and hypercarbia.
Open pneumothorax-therapy • Temporary management of this injury includes covering the wound with an occlusive dressing that is taped on three sides. • This acts as a flutter valve, permitting effective ventilation on inspiration while allowing accumulated air to escape from the pleural space on the untaped side, so that a tension pneumothorax is prevented. • Definitive treatment requires closure of the chest wall defect and tube thoracostomy remote from the wound.
Flail chest • Flail chest occurs when three or more contiguous ribs are fractured in at least two locations. Paradoxical movement of this free-floating segment of chest wall may be evident in patients with spontaneous ventilation, due to the negative intrapleural pressure of inspiration.
Flail chest • Rarely the additional work of breathing and chest wall pain caused by the flail segment is sufficient to compromise ventilation. • However, it is the decreased compliance and increased shunt fraction caused by the associated pulmonary contusion that is typically the source of postinjury pulmonary dysfunction.
Flail chest • Pulmonary contusion often progresses during the first 12 hours. Resultant hypoventilation and hypoxemia may require presumptive intubation and mechanical ventilation.
A B Flail chest-therapy • The patient’s initial chest radiograph often underestimates the extent of the pulmonary parenchymal damage; • Close monitoring and frequent clinical re-evaluation are warranted
Circulation with hemorrhage control • With a secure airway and adequate ventilation established, circulatory status is the next priority. • An initial approximation of the patient’s cardiovascular status can be obtained by palpating peripheral pulses. • In general, systolic blood pressure (SBP) must be 60mmHg for the carotid pulse to be palpable, 70 mmHg for the femoral pulse, and 80 mmHg for the radial pulse.
Circulation with hemorrhage control • At this point of patient evaluation, any episode of hypotension (defined as a SBP <90 mmHg) is assumed to be caused by hemorrhage until proven otherwise. • Patients should be closely monitored until normal vital sign values are restored.