Download
1 / 58
870 likes | 2.35k Vues
Vaccines to Prevent Ocogenic HPV Infections John Schiller, National Cancer Institute, NIH, USA HPV and Cancer Prophylactic HPV Vaccine Implementation Issues.

E N D
Vaccines to Prevent Ocogenic HPV Infections John Schiller, National Cancer Institute, NIH, USA HPV and CancerProphylactic HPV VaccineImplementation Issues
Worldwide incidence and distribution of cancers attributable to HPVCervix had approximately 450,000 HPV and total casesOropharnyx has 50,000 HPV cases and 100,000 total casesAnus has 40,000 HPV and 50,000 total casesOral has 25,000 HPV and 250,000 total casesLarynx has 20,000 HPV and 150,000 total casesVulva has 10,000 HPV and 30,000 total casesPenis has 10,000 HPV and 30,000 total cases
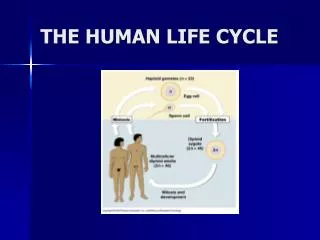
The HPV Life Cycle JA Kahn, NEJM, 2009;361:271
Female reproductive Tract Anatomy & Histology Initiation Site of Cervical Cancers
Transformation Zones in Other HPV Cancers Anal cancer also occur at the transformation zone.HPV Infections of the vulvar, vagina and penis are common.Cancers at these site are relatively rare.They lack a transformation zone.
Cervical Cancer Develop at the Transition ZoneBetween Squamous and Columnar Epithelium
Rate HPV Precancer Cancer 15 y.o. 30 y.o. 45 y.o. Age Time Line of Cervical HPV InfectionsAnd Progession to Cervical Cancer • Lifetime incidence of genital HPV infection >80% in U.S. • Most infections clear spontaneously, eliminating cancer risk for that infection. • Persistent infection with a high-risk HPV, especially HPV16 or 18, is the single most important risk factor for progression to precancer and cancer.
5 Most Common HPV Types in Squamous Cell Carcinoma - By Region
HPVs Cause A Variety of Proliferative Diseases EV cutaneous, mostly asymptomatic foot warts HPV16 mucosal, cancer- associated hand warts HPV18 HPV11 HPV6 genital warts
Therapeutic vs Prophylactic HPV Vaccines • Therapeutic vaccine attractive since Cervical CA develops slowly from well defined and routinely identified viral lesions. E6 and E7 expressed. • Approved vaccines against other viral infections are preventive (based on neutralizing antibodies), not therapeutic (based on cell mediated immune responses). • We initially concentrated on Prophylactic Vaccines
Live Attenuated Viruses Are Not SuitableFor an HPV Prophylactic Vaccine• Papillomavirus cannot be efficiently grown in cultured cells• The viral genomes contain oncogenes• Virion protein-based subunit vaccines are preferable, if they could efficiently induce neutralizing antibodies.
Papillomaviruses Encode Two Structural Proteins Papillomavirus Particle • L1: the major structural protein. Each viral particle has 360 copies in 72 pentamers. • L2: the minor structural protein. Up to 72 copies per particle. L1 L1 L2 L1 L1 L1
Key To the Development of L1 Vaccines IM injection of virions, but not denatured L1 or L1 pepptides, induced protection from experimental infection in animal models. Generating an immunogen with conformationally correct L1 was critical.
Prophyactic HPV Vaccines Are L1 Virus Like Particles (VLPs) L1 Insertion in Baculovirus Expression VectorProduction inInsect CellsSpontaneous assemblyof L1 into VLPsInduce high titersof virion neutralizingantibodies HPV Virion L1 coding region
Two Distinct HPV VLP Vaccines Were Developed Commercially GlaxoSmithKline: HPV16Cervarix HPV18 ASO4 Adjuvant (Aluminum + MPL) Made in insect cellsMerck: HPV16Gardasil HPV18 HPV6 HPV11 Aluminum Adjuvant Made in yeast IM Injections at 0, 1 or 2, and 6 months
Efficay Endpoints in Clinical Trials Cervical intraepithelial neoplasia (CIN): CIN1, CIN2, CIN3Cervical adenocarcionoma in situ (AIS)External genital lesions (EGL): genital warts, vulvar/vaginal dysplasia-GardasilIncident or persistent vaccine type infection: cervical HPV DNAMost analyses restricted to HPV types in the vaccines Endpoint for Licensure:CIN2+ from incident infection by vaccine type
HPV Vaccine Phase III Trial Outcomes: Interim ATP Analyses - Vaccine Types Only Young women without prior infection with vaccine included HPV types
HPV Vaccine Efficacy Trial Outcomes Efficacy measured as prevention of incident (new) infection and disease caused by the HPV types in each vaccine (fully vaccinated women, 16-26 years old) ●Garland (2007) used the 6/11/16/18 vaccine and using CIN2/3, AIS, GW, Vin and VAIN as endpoints found that the vaccine efficiency was 100% (94-100). ●Kjaer (2009) used the 6/11/16/18 vaccine and using CIN2/3, AIS, VIN2/3 and VAIN2/3 as endpoints found that the vaccine efficieny was 98% (93-100). ●Paavinen (2009) used the 16/18 vaccine and using CIN2/3 as an endpoint found that the vaccine was 98% efficient (88-100).
Efficacy of Less than Three Doses of Cervarix NCI’s Costa Rica TrialProtection from 12 mo. Persistent HPV16/18 Infection*●With 3 doses the vaccine efficacy is 80.9% (70.1-89.8).●With two doses the vaccine efficacy is 84.1% (50.2-96.3). ●With one dose the vaccine efficacy is 100% (66.5-100).
Cumulative Incidence of All CIN2+ Regardless of HPV DNA or Sero-Status at Entry Intention to Treat Cohort PATRICIA - Cervarix Study Placebo Cervarix
Gardasil Approval SpecificsUS FDA approved for 9-26 yr old females in June ‘06 European Union and Australia approved for: 9-26 yr old females 9-15 yr old boysApproval in 9-15 yr old girls and boys was based on immunogenicity bridging studies not efficacy
Cervarix Approval Specifics E.U.: 10-25 yr old females in 2007 Australia: 9-45 yr old females in 2007 U.S. FDA approved for 10-25 yr old females in Oct. ’09Approval in 9-15 yr old girls and 26-45 yr old women was based on immunogenicity bridging studies not efficacy
ATP Analysis of PATRICIA (Cervarix):Vaccine Efficacy Against 6 Months Persistent DNAHPV-16/18 93.8%HPV-31 78.7%HPV-33 45.7%HPV-45 75.7%HPV-52 7.8%HPV-58 1.8%HR except 16/18 12.1%Any HR type 25.0%
Neutralize Ab Response to L1 is Predominately Type-Specific Anti-L1 antibodies are generated against conformational surface loops HPV11 HPV35 HPV16 HPV18
Percentages of cervical cancer cases arrributed to the most frequent HPV types in all world regionsHPV-16 54.6%HPV-18 15.8%HPV-33 4.4%HPV-45 3.7%HPV-31 3.5%HPV-58 3.4%HPV-52 2.5%HPV-35 1.8%HPV-59 1.1%HPV-56 0.8%HPV-51 0.7%HPV-39 0.7%HPV-73 0.5%HPV-68 0.5%HPV-82 0.2%
Potential Impact of the Vaccines in the US 10,000,000 have subclinical HPV infection in US1,400,000 have low-grade dysplasia300,000 have high-grade dysplasia10,000 have cancer
Efficacy of Gardasil in Mid-Adult WomenAges 24-45 Against Vaccine Types Persistent infection, CIN or EGF has 88.7% efficiency (78.1-94.8)Persistent infection has 89.6% efficiency (79.3-95.4)CIN-any grade has 94.1% efficiencyCIN 2/3 has 83.3% efficiency (37.6-99.6)EGF has 100% efficiency (30.8-100)
Rate Reduction in Treatment Related to Any HPV Type in Gardasil-Vaccinated Mid-Adult Women Coposcopy has a 4.7% rate reduction (-9.5-17.1)Biopsy has a 3.7% rate reduction (-11.0-16.4) Definitive therapy has a 8.8% reduction (-16.7-28.8)
Gardasil Prevents Genital Warts in Young Men Ages 16-26External genital lesionsHPV-6, 11, 16, 28 90.4%Any type 83.8%AIN-any gradeHPV-6, 11, 16, 18 77.5%Any type 54.9%HPV-58 1.8%AIN 2/3 74.9%Persistent anal infectionAny HPV- 6, 11, 16, 28 94.9%
Gardasil: Time to HPV6/11/16/18-Related AIN in MSM:Per Protocol Efficacy Population Number of Events 77.5 % Efficacy Months in Study
Anal and Cervical HPV16/18 VE Among Women w/out Evidence of Cervical HPV DNA at Vaccination Costa Rica Trial of Cervarix Efficacy at Study Exit Against HPV DNA by SiteAnus: The HPV arm had 0.8% HPV 16/18 prevalence.Anus: The control arm has 4.9% HPV 16/18 prevalence. The HPV 16/18 VE was 83.6% (66.7-92.8). Cervix: The HPV arm had 1.0% HPV 16/18 prevalence.Cervix: The control arm has 8.2% HPV 16/18 prevalence. The HPV 16/18 VE was 87.9% (77.4-94.0). p = 0.55
December 2010 AIN in MSM Study has led to FDA approval of Gardasil for the prevention of anal cancer and AIN in both men and women. Gardasil approved for Genital Warts in 2009
United States: Incidence and Distribution of Cancers Attributable to HPV Infection●There are about 10,000 cases of cervix cancer and all are HPV cases●There are about 3,000 cases of vulva/vagina cancer and 50% are HPV cases ●There are about 3,000 cases of anus cancer and 90% are HPV cases ●There are about 500 cases of penis cancer and 20% are HPV cases ●There are about 8,000 cases of oropharynx cancer and all are HPV cases
Clinical Trial Evidence for Vaccine EfficacyAgainst Infection/IN at Site. The vaccine is effective against cervix cancer, vulva/vagina cancer, anus cancer and penis cancer but not oropharynx cancer
Consistency of Antibody Response to VLPsPercent of Women Serocoverting to Individual HPVVLPs in Merck Quadravalent VLP Vaccine Gardasil* HPV6 99.8% HPV11 99.8% HPV16 99.8% HPV18 99.5%*4666 women vaccined 3 times by intramuscular injection
Durability of Antibody Response to Cervarix 0 7 12 18 25 33 39 45 51 57 63 69 75 Month: 0 7 12 18 25 33 39 45 51 57 63 69 75 Month: HPV16 VLP ELISA HPV16 Neutralization Assay
Duration of Protection Strong Protection through the six years since the studies began. No evidence for increase numbers of breakthrough infections.
How Could IM Injection of a VLP VaccineInduce a Protective Ab Response at the Cervix? Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
T Cell Responses To L1 Unlikely to Induce Regression:Virion Protein Expression is Lost During Progression CIN 1 CIN 2 CIN 3 Decreasing Epithelial Differentiation Virus Producing Non-productive Non-productive Doorbar, J Clin Virol 32:7-15, 2005
VLP Vaccines Don’t Influence Prevalent InfectionNCI/Costa Rican HPV16/18 VLP Vaccine Trial :Rate of HPV-16/18 DNA Clearance by Treatment Arm VE = -5.4% VE = 5.8%
Conclusions: HPV VLP Vaccine Efficacy • VLP vaccines are highly effective at protection against a spectrum of anogenital HPV endpoints from incident infection to high grade precancer.• Gardasil is also highly protective againstgenital warts in women and men.• Protection is type-restricted, consistent with protection being antibody mediated.• Duration of protection is unknown, but strong protection at 6 years, after antibody levels havereached a plateau, is very encouraging
Who Should Be Vaccinated?In descending order of importance:10-14 year old girls - the ultimate target group since they have not yet been exposed to these sexually transmitted viruses Sexually active women - since many may not yet been exposed to at least one of the vaccine types; may reduce transmission - increase herd immunity Adolescent boys and men - only 8% of HPV cancer in men; may be small impact on herd immunity if coverage of women high; most models suggest male vaccination would not be cost effective
Acquisition of Genital HPV Infection in Young Women With Their First Sexual Partner 70 60 50 Cumulative risk of HPV (%) 40 30 N=242 (15-19 years old, UK) 20 10 0 Time since first intercourse (months) 0 12 24 36 48 60
Who Should Be Vaccinated?In descending order of importance:10-14 year old girls - the ultimate target group since they have not yet been exposed to these sexually transmitted viruses Sexually active women - since many may not yet been exposed to at least one of the vaccine types; may reduce transmission - increase herd immunity Adolescent boys and men - only 8% of HPV cancer in men; may be small impact on herd immunity if coverage of women high; most models suggest male vaccination would not be cost effective
Recommendations for HPV Vaccination in Females as of October 2007 From: Tom Wright, HPV Today, February 2008
Who Should Be Vaccinated?In descending order of importance:10-14 year old girls - the ultimate target group since they have not yet been exposed to these sexually transmitted viruses Sexually active women - since many may not yet been exposed to at least one of the vaccine types; may reduce transmission - increase herd immunity Adolescent boys and men - only 8% of HPV cancer in men; may be small impact on herd immunity if coverage of women high; most models suggest male vaccination would not be cost effective
October 2011CDC Advisory committee recommendsthat boys ages 11-12 be routinely vaccinated with Gardasil, with catch up through age 26.
Genital Wart Time Trends in Australian Women 2004-2009 59% 2004 2005 2006 2007 2008 2009 2004 2005 2006 2007 2008 2009