Download

1 / 38
480 likes | 1.4k Vues
SEX DETERMINATION AND DIFFERENTIATION. Lots to talk about. Gender Determination Gender Differentiation Gonads Brain Gender Differences in the HPG axis Menstrual Cycle Male Gonadal Hormone Regulation Disorders of Sexual Differentiation. Sexual Determination. Chromosomal sex : XX XY

E N D
SEX DETERMINATION AND DIFFERENTIATION
Lots to talk about . . . • Gender Determination • Gender Differentiation • Gonads • Brain • Gender Differences in the HPG axis • Menstrual Cycle • Male Gonadal Hormone Regulation • Disorders of Sexual Differentiation
Sexual Determination • Chromosomal sex: XXXY • Determines gonadal sex • Determines hormonal sex Gonadal differentiation occurs during the 5th and 6th weeks of fetal development . . .
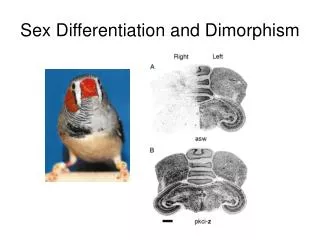
Sexual Differentiation • A complex process . . .
Sexual Differentiation A masculine-feminine continuum . . . • Masculinization = induction of male traits. • Defeminization = removal of the potential for female traits. • Feminization = induction of female traits. • Demasculinization = removal of the potential for male traits.
Sexual Differentiation • Androgens are responsible for the differentiation of the external genitalia . . . • Androgens Testosterone 5α-reductase DHT penis, scrotum • No Androgens clitoris, vaginal labia In the absence of androgens, the “default” gonadal development is FEMALE
Temperature-dependent Sex Determination? • Reptiles & Fish: Temperature of egg incubation is an important factor in determining gender!! • Lizards / Alligators: Temperatures > 30° C produce males and < 28° C produce females in some lizards and alligators!! Temperatures may inactivate enzymes like aromatase and 5α-reductase. • And humans? The DMRT1 gene required for male development in humans and mice is similar to the mab-3 and doublesex genes of animals whose sex is determined by temperature . . . An evolutionary link? Cool!! Hot!
Sexual Differentiation of the Brain • The POTENTIAL for feminine or masculine behavior appears to be organized by early exposure to hormones. Like the body, the brain is initially programmed to develop in the FEMALE direction.
+ Sexual Organization of the Brain Creation of the male rat brain GONADSTestosterone reductase aromatase Dihydrotestosterone Estrogen Androgen-receptor Estrogen-receptor
Sexual Organization of the Brain Creation of the female rat brain GonadsEstrogen Female : less testosterone to access brain and aromatize to estrogen so again, no possibility of masculinization Estrogen Sequestered by alpha-fetoprotein End-result : Estrogen is removed from placenta and metabolized by maternal liver Less estrogen to get to brain and defeminize the brain
Summary: Sexual Organization of the Brain • Male Rats: Testosterone aromatized to estrogen (E) appears to be especially important for masculinizing the male rat brain!! • Female Rats: Exposed to high levels of E from mom’s ovaries and own E from fetal ovaries, so why are they not masculinized? • Mom has high levels of the carrier protein α-fetoprotein in circulation which binds estrogens well, but NOT androgens. • Αlpha-fetoprotein sequesters, or removes, E via the placenta to be metabolized by mom’s liver. It protects the female rat brain from any masculinizing effects of E.
Sexual Organization of the Brain GONADSTestosteroneEstrogen reductase aromatase Estrogen Sequestered in brain by alpha-fetoprotein Dihydrotestosterone Estrogen Any dysfunction in genetic and hormonal pathways will lead to problems in sexual differentiation in both animals and humans . . .
Gender Differences in HPG regulation Back to the axes . . . - GnRH Pulsatile Release - LH/FSH Pulsatile Release - Sex Steroids
Gender Differences in HPG Regulation • Females: Cyclic gonadal function • Estrogens and Progesterone • Males: Tonic gonadal function • Testosterone How does this happen?
Secretion of Sex Steroids - GnRH Pulsatile Release Surge + - LH/FSH + Pulsatile Release (every 60 mins for humans) - Sex Steroids Females : Steady Increase in Estrogen How??? The more estrogen you have, the higher the probability to induce POSITIVE FEEDBACK and surges of GnRH and LH / FSH.
What do you predict? - GnRH + OVX + low doses Estrogen - LH/FSH + LH GnRH OVX + high doses Estrogen LH - Sex Steroids GnRH Conclusion : High doses of estrogen in females overcomes negative feedback
.. evidence that this only applies to females - GnRH + Castration + low doses Estrogen - LH/FSH + LH GnRH Castration + high doses Estrogen LH - Sex Steroids GnRH Conclusion : High doses of estrogen in females overcome negative feedback
Amazing Ovarian Function • 1-2 million follicles in each ovary at birth only about 400 oogonia (potential ovum) used during female reproductive lifespan! • Ovulation is a result of a careful orchestration of LH, the FSH:LH ratio, receptor systems, and the availability of estrogens, androgens, plus other neurochemicals (eg., inhibin – a peptide that feeds back to inhibit FSH)
Follicular Phase Follicular cell Stimulated by FSH Produces estradiol and other estrogens E synthesis hypothesis . . . Thecal cells surrounding the follicle have LH receptors and produce androgens Granulosa cells surrounding the follicle have FSH receptors and convert androgens to estradiol Luteal Phase Corpus Luteum An endocrine gland Produces progesterone (and some estrogen) Progesterone suppresses LH and GnRH Progesterone down-regulates estradiol receptors Capillaries in the endometrial lining constrict when E and P rapidly withdraw on days 27-28, leading to menstruation. Quick Facts about Ovarian Function
How about Testicular Function? • Testes produce many trillions of spermatozoa in a lifetime! • Leydig cells: • Have LH receptors • Produce testosterone • Initiate paracrine interactions with seminiferous tubules and Sertoli cells to influence spermatogenesis. • Sertoli cells: • Have FSH receptors • Produce estradiol from testosterone • Produce proteins like androgen-binding protein, nourish developing spermatozoa, phagocytosis of damaged sperm, produce sperm transport fluid.
Disorders of Sexual Differentiation Experiments of nature . . . HERMAPHRODITE : A person born with both male and female sex organs. This is a vague, confusing and inaccurate definition. There are 3 labels of Hermaphrodites: True, Male Pseudo and Female Pseudo. PSEUDOHERMAPHRODITE : Human babies born with ambiguous genitalia. Usually one set of gonads is present. http://users.southeast.net/~help/sexdiff.html
Disorders of Sexual Differentiation TRUE HERMAPHRODITE A person born with both ovary and testicular tissue, this could be 2 separate gonads ( one of each) or a combination of both in one (an ovotestes). The chromosome compliment can be XX (female), XY (male), XX/XY (mosaic) or even XO (extremely rare). Those XX with female genitalia are raised female (some have even given birth). Those XY with male genitalia are raised male ( a few have fathered children). The children born XX/XY or XO (with genitalia male or female are raised in the sex they look most like). Those born with ambiguous genitalia have many medical tests for the doctors to determine which sex they should be assigned. Doctors then recommend early surgery to make the child look physically like the sex assigned to them. CAUSES: The causes are not known, The medical community does know this is a very rare condition but do not have accurate figures to how many people have this condition (depending on the literature between 350-450 known cases).
Disorders of Sexual Differentiation 2. FEMALE PSEUDO A person born XX with normal female internal organs but with "masculinized" genitalia. They can appear more male than female or a combination of each. CAUSES The most common is Congenital Adrenal Hyperplasia (CAH) it occurs approximately 1:14,000 births.This is when the adrenal glands overproduce testosterone. It also has been recorded that some persons with this disorder had been exposed to progesterone-like drugs before they were born (diethylstilbestrol and medroxyprogesterone acetate used to maintain pregnancies). No cure as of today, but treatment is available (cortisol).
Disorders of Sexual Differentiation 3. MALE PSEUDO A person born XY with testes (usually in the abdominal cavity). The external genitalia are usually female but can be ambiguous. CAUSES The most common cause is Androgen Insensitivity Syndrome (AIS). This is when the body doesn't respond to the androgen being produced because the androgen receptors do not function. There are different variations: Complete (CAIS) , and Partial (PAIS). This condition has a variety of names and occurrence rates.
Disorders of Sexual Differentiation Another related syndrome : Turner Syndrome A disorder in women caused by an inherited chromosomal defect. This disorder inhibits sexual development and causes infertility. Ovarian development is impaired, preventing gonadal estrogen and androgen production!! Cause : Abnormality in or absence of the second X chromosome. It affects 1 out of 3,000 live births. There are many manifestations of this syndrome: -Short Stature -Webbing of the skin of the neck -Absent or retarded development of secondary sexual characteristics -Absence of menstruation
Female Advantages: Verbal tasks Perceptual Skills Fine Motor Skills Mathematical Calculation Male Advantages: Quantitative tasks Directed Motor Skills Visuospatial Abilities Mathematical Reasoning Gender Dimorphism in Cognitive Function
TS Cognitive Findings . . . Normal verbal skills Impaired visual-spatial ability Impaired visual-perceptual ability Nonverbal memory < Verbal memory Impaired on attention tasks Impaired on tests of arithmetic Impaired on tests of motor function A unique sex hormone-deficient model that can be be used to investigate hormone effects on cognition.
Estrogen Treatment for TS Girls . . . Ross et al., 2000 Double-blind, placebo controlled study: 29 children (7-9 years) controls placebo GH GH / E estrogen RESULTS: Controls > Estrogen-treated girls > Placebo girls on recall of word lists (verbal memory) . . . But only the difference between normal controls and placebo girls was significant; also small sample size, low E-dose . . .
Androgen Treatment for TS Girls . . . Ross et al., 2003 Double-blind, placebo controlled study: 51 children (10-14 years) controls placebo/GH Oxandrolone / GH (androgen that does not aromatize to estrogen) RESULTS: Androgen group > placebo on tests of working memory over two years of treatment. No differences on tests of verbal ability, spatial cognition, and executive function. BUT, effects of GH? practice effects of testing twice? . . .
Other Clinical Neuroendocrine Models • PCOS (Polycystic Ovary Syndrome) • Transsexual studies . . .