Download
1 / 40
400 likes | 501 Vues
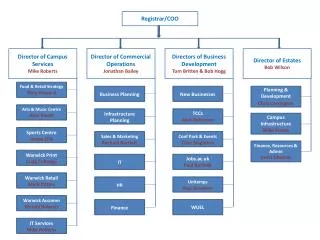
UA Choice Mike Humphrey Director of Benefits October 2007. Shifting Costs. Reducing Cost. Changing Delivery. Employer Responses. Employees. Managed Care. Plan Change & Wellness Programs. Employers Responses. Shift the Cost (“squeezing the balloon”) Benefit cutbacks – higher deductibles

E N D
Shifting Costs Reducing Cost Changing Delivery Employer Responses Employees Managed Care Plan Change & Wellness Programs
Employers Responses • Shift the Cost (“squeezing the balloon”) • Benefit cutbacks – higher deductibles • Employers contribute less toward the plan cost • Employee charges for coverage are increased • Change the Delivery System • Managed Care, Open & Closed Networks • High Performance Networks • Reduce the Cost (“deflating the balloon”) • Contract with Medical Providers to take less • Wellness initiatives • Disease management
University Health Care Trends Beyond 2007Are they sustainable?
Current UA Support Programs In Place Health & Wellness
UA’s Health Programs • Case Management – for the seriously ill • Disease Management – for the chronically ill • Health Risk Assessment • Wellness/Life Style Coaching • On Site Wellness Programs • Pharmacy Program Management
Disease Management Principles and Goals • Improve the health and increase the quality of life of UA employees and dependents • Support the physician / patient relationship • Improve employee productivity • Reduce total health care costs
2006 Program Diabetes Heart Failure Coronary Artery Disease 2007 Program Diabetes Heart Failure Coronary Artery Disease Low Back Pain Osteoporosis Osteoarthritis Hepatitis C Urinary Incontinence Pressure Ulcers Atrial Fibrillation Inflammatory Bowel Disease Irritable Bowel Syndrome Fibromyalgia Acid Related Disorders UA’s Disease Management Program
2006 Program Number of participants – 431 Costs avoided – $493,000 2007 Program Number of participants – 2,100 est. Costs avoided – $723,000 est. UA Disease Management Opportunity Analysis
Preventable claims costGroup Level health care expenditures Depression Stress Blood Sugar Smoking Obesity Blood Pressure Sedentary Life N = 46,026 X 6 years Source: Anderson, et. al., (2000, Sept/Oct). The Relationship Between Modifiable Health Risks and Group-Level Health Care Expenditures, AJHP, 15(1), p. 45-52.
Health risks push costs upYet preventable through lifestyle change Average annual per capita excesshealthcosts when risk is present. Goetzel, R et al. The Relationship Between Modifiable Health Risks and Health Care Expenditures, Journal of Occupational and Environmental Medicine. 1998;10:843-854
Effect of Single Risk Factors Health Plan Cost Percent Higher Annual Health Plan Costs Source: Goetzel RZ, et. al. (1998, October). The relationship between modifiable health risks and health care expenditures: An analysis of the multi-employer HERO health risk and cost database. JOEM, 40(10):843-54.
Effects of Health Risks on Absenteeism Sick Leave Absenteeism Percent Higher Absenteeism Source: Serxner, S., et al., (2001). The impact of behavioral health risks on worker absenteeism. JOEM, 43(4), 347-354
UA’s Phase 1“Virtual” Program With WebMD Referrals
WIN for Alaska Health In Action Program
Increase awareness of health risks Reduce the number of health risks Increase participation in healthy behaviors Provide a supportive environment for lifestyle changes Increase employee satisfaction and morale UA’s On Site Wellness ProgramWith WIN For Alaska – Goals
UA’s Phase 2 Program With WebMD & WIN For Alaska Virtual Site-based
PharmaCare’s Observations PharmaCare (Caremark) reviewed last years prescription drug utilization and performance The factors most impacting plan cost are • Member Utilization – the number of medications • Product Mix – name brand vs. generic • Plan Design – name brand vs. generic cost Of these three key areas, plan design offers the greatest opportunity for impact.
PharmaCare Summary • 44% of participants are utilizing the plan • PharmaCare standard book of business approximately 33% take advantage of the plan. • This high utilization is reflective of the rich benefit offered. • Within the Standard plan, 84% of UA’s utilizing population can be found. • They process 70% of total Rx’s and account for almost 75% of the total plan cost.
July 1, 2007 to June 30, 2007 Product Mix Univ. BoB: Retail: $61.55 Mail: $191.41 Univ. of Alaska: Retail: $63.72 Mail: $249.05 Univ. BoB: Brand Rx: $138.19 Generic Rx: $24.07 Univ. of Alaska: Brand Rx: $131.88 Generic Rx: $25.59
PharmaCare Recommendations • Increase the promotion of generics • Move to a uniform three tier plan design for all plans (Deluxe, Standard and Economy) • Update the plan copays and coinsurance • Implement 30 day supply limit for specialty med to prevent waste • Add standard prior authorization and quantity limits • Addition of a member educations program designed to highlight the true cost of the prescription program (Script Summary)
PharmaCare Recommendations • Expand Brand / Generic copay differential • 3,200 Brands w/gen alternatives • Avg cost savings $100 per generic • Change preferred name brands to a coinsurance percentages to help plans keep pace with inflation • Addition of 3rd tier non formulary brand to increase generic and preferred name brand use
RecommendationsPlan Design • Generic $5.00 • Lower generic copay results in direct cost, but should encourage more generic use • Preferred Name Brand 80/20% • Help increase the use of name brands with the best discounts • Non-Preferred Name Brand 70/30% • Steer participants away from medications with little discount • Combined savings to the Pharmacy Plan • $578,000 -- over 12.3%
PharmaCare Recommendations • Implement 30 day supply (DS) limits for specialty medications to prevent waste • Relocate distribution center to Seattle • Estimated waste = $160,000 • PharmaCare reports – 42% of patients using the specialty pharmacy say they are better able to manage their condition and their medications
PharmaCare Recommendations • Adjust $500 individual pharmacy out-of-pocket maximum to $1,000 for specialty medications • 1% to 5% reduction plan cost = $66,000 - $330,000 annually
PharmaCare Recommendations Implement Industry Standard Prior Authorizations and Quantity Limits • Over a dozen eligible Prior Authorization classes • Cosmetic Acne/Skin/Dermatological – YTD Spend $83,000 • 1% to 3% savings opportunity = $66,000 to $199,000 total plan cost • Quantity Limit options for three growing classes of meds = savings @ $.10 pmpm • Implement without the option to grandfather existing patients • $.10 pmpm x 9500 mbrs = $950 month x 12 = $11,400 savings opportunity
PharmaCare Recommendations Total annual pharmacy plan costs avoided (saved) $950,000
Proposed FY 09 Health Plan Changes This is a link to an Excel file named FY 09 health plan