Download
1 / 18
180 likes | 185 Vues
EP-125. Brainstem disconnection: two additional patients and expansion of the phenotype. Andrea Poretti 1,2 , Thierry A.G.M. Huisman 1 , Eugen Boltshauser 2 1 Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H Morgan

E N D
EP-125 Brainstem disconnection: two additional patients and expansion of the phenotype Andrea Poretti 1,2, Thierry A.G.M. Huisman 1, Eugen Boltshauser 2 1Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD 2Department of Pediatric Neurology, University Children’s Hospital of Zurich, Switzerland ASNR 53rd Annual Meeting, Chicago, April 25-30, 2015
Disclosure • We have nothing to disclose • No relevant financial relations interfering with our presentation
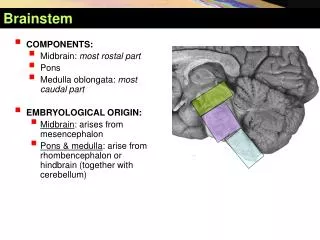
Brainstem disconnection (BD) • Rare posterior fossa congenital abnormality • Only 12 children with BD reported so far • Diagnosis based on typical neuroimaging findings: • Nearly complete absence of a brainstem segment with the intact rostral and caudal brainstem portions connected only by a thin cord of tissue Poretti A et al, Neuropediatrics, 2007
Brainstem disconnection • Neuroimaging classification based on the location of the disconnection: • Ponto-mesencephalic • Ponto-medullary • Ponto-cervical • Outcome = poor • The majority of children died within the first two months of life • No developmental milestones achieved 1 2 3 Bednarek N et al, Eur J Paediatr Neurol, 2005; McCann E et al, Pediatr Radiol, 2005; Okumura A et al, Am J Med Gen A, 2009
Purpose • To report on: • Clinical presentation + outcome • Imaging • Genetics • Neuropathology in 2 children with a milder phenotype of BD to extend the phenotypic spectrum of this very rare congenital abnormality
Methods • Clinical findings & outcome: from clinical history & follow-up examinations • Neuroimaging: qualitative evaluation of brain MRI for infra-/supratentorial abnormalities • Genetic analysis • Neuropathology examination (n=1)
1. Clinical findings • Patient 1 (male): • At birth: global hypotonia, reduced left facial movements, feeding difficulties requiring a nasogastric tube • Unstable body temperature (32.5-42.5°C), generalized seizures, brief visual fixation, required a gastrostomy tube, no auditory brainstem evoked responses • Patient 2 (female): • At birth: impaired mouth opening, unilateral preauricular tag, long gap esophageal atresia (type Vogt IIIB) • Epileptic seizures since the age of 2 weeks, unstable body temperature (33.7-42.0°C), required a gastrostomy tube
1. Outcome • Patient 1: • At 8 months of age: smiled, targeted reaction after a tactile stimulus, moved all extremities spontaneously and symmetrically, brought hands to the mouth • Died at 8 months of age because of pneumonia • Patient 2: • At 14 months of age: development of hydrocephalus no VP-shunt because of palliative situation • At 4.5 years of age (alive): no visual contact, no spontaneous movements, generalized spasticity, no developmental milestones have been reached
2. Imaging: Patient 1 (A) Midsagittal and (B) coronal T2-weighted brain MR images at 3-weeks show a markedly small pons with only a thin strand of tissue (arrow) anteriorly connecting the spared upper portion of the pons and the medulla. The cerebellar vermis and hemispheres are globally hypoplastic
2. Imaging: Patient 2 (A) Midsagittal T2-weighted, (B) coronal FLAIR, (C) and (D) axial T2-weighted MR and (E) time-of-flight MRA images at 3 weeks reveal absence of the middle and lower pons with only two thin strands of tissue (arrows) anteriorly and posteriorly connecting the upper pons and the medulla. The cerebellar vermis and hemispheres are globally hypoplastic. The basilar artery is not visible.
2. Imaging: Patient 2 A chest radiograph shows partial fusion of the posterior right 3/4/5 ribs and butterfly shape/ hemivertebra of the thoracic spine. Prominent cardio-thymic silhouette.
3. Genetic findings • Patient 1: Whole exome sequencing: • Heterozygosity for a p.Thr30Ala (c.88-A>G) variant in exon 3 in the BMP4 gene = inherited from the father • Hemizygosity for a p.Arg293Gln (c.878-G>A) variant in exon 7 in the SEPT6 gene on the X chromosome = inherited from the mother and also found in the oldest healthy brother Both variants are not causative for BD • Patient 2: Array comparative genomic hybridization (CGH): • No copy number variants
4. Neuropathology: Patient 1 • Brainstem: nearly-normal midbrain, small superior cerebellar peduncles, absent medial lemnisci, short and small pons (mostly tegmentum, only a thin rim of basis pontis), dysplastic medulla • Cerebellum: hypoplasia of the vermis, otherwise normal • Normal cerebral hemispheres • Normal vertebral and basilar arteries, no gliosis in the areas supplied by the posterior circulation Axial histologic section of upper pons and cerebellum. Luxol Fast Blue/H&E combination stain, 1x original magnification. Courtesy of Dr. D.C. Miller, University of Missouri, Columbia, MO
Discussion: Phenotype • Survival: • 10 of 12 children reported: died < 2 months of age • Our patients: survived longer (8 months and >4.5 years) • Last follow-up: • Children who survived > 2 months: still hospitalized (5 months and 4 years of age), mechanical ventilation/ tracheostomy, gastrostomy, no development • Our patients: no mechanical ventilation, patient 1 = only BD patient who achieved developmental milestones Our patients = milder phenotpye
Discussion: Pathomechanism Malformation (pro) Disruptive (vascular) lesion (pro) Models with missing hindbrain segments: remaining segments always contiguous (≠ in BD) Early vascular disruptions tissue liquefaction without gliotic scars Association with syringomyelia progressively insufficient perfusion due to hypoplastic basilar artery and obstructed venous drainage due to abnormal glial barrier around the posterior brainstem Negative genetic analysis (?) • A EN2 murine model: agenesis of mesencephalon and metencephalon; mutations in EN2, however, not found in 2 children with BD • Presence of additional brain malformations, dysmorphic features, and extracerebral involvement Sarnat HB et al, Pediatr Dev Pathol, 2002; Barth PG et al, Neuropediatrics, 2008
Conclusions • Although the long-term neurodevelopmental outcome of BD remains unfavorable, the expansion of the phenotypic spectrum may be important in terms of family counseling • It remains unknown whether BD is genetically driven (malformation) or is the outcome of a prenatal (most likely vascular) disruptive insult
Acknowledgments • Dr. Douglas C. Miller, Department of Pathology and Anatomical Sciences, University of Missouri School of Medicine, Columbia, Missouri, United States for sharing neuropathology data of Patient 1 • The families of the affected children for supporting this presentation